Surgical Treatment of Abdominal Aortic Aneurysm in a 3-Year-Old Girl with Tuberous Sclerosis Complex
Surgical Treatment of Abdominal Aortic Aneurysm in a 3-Year-Old Girl with Tuberous Sclerosis Complex
A B S T R A C T
The tuberous sclerosis complex is a multisystem disorder affecting children and adults. The association between abdominal aortic aneurysm and tuberous sclerosis is rare. We present 3-year-old girl with a pulsatile abdominal mass in the pediatrician´s medical review. An abdominal evaluation showed a 6cm infrarenal abdominal aortic aneurysm. The patient underwent open repair with a 14-mm Dacron tube graft. The histological examination revealed connective tissue proliferation, fibrosis, and calcification of the aortic wall. Frequent follow-ups with ultrasounds showed no alterations. Due to the high risk of rupture, early surgical repair is the first-line therapy.
Keywords
Tuberous sclerosis, abdominal aortic aneurysm, congenital heart disease (CHD), vascular disease, genetics
Introduction
Tuberous sclerosis (TS) is an autosomal dominant disease arising from genetically programmed hyperplasia of ectodermal and mesodermal cells and manifested by a variety of lesions in the skin, central nervous system, heart, kidney, and other organs, affecting children and adults [1]. The association between abdominal aortic aneurysm (AAA) and tuberous sclerosis is rare. Diagnostic noninvasive vascular evaluation must include ultrasound, magnetic resonance angiography and computed tomography [2, 3]. We present 3-year-old girl with a pulsatile abdominal mass in the pediatrician´s medical review. An abdominal evaluation showed a 6cm infrarenal AAA. We present our experience on the open repair of AAA in a girl with TS.
Case Report
A 3-year-old girl with normal growth and development with history of partial seizures and no significant medical history nor a familiar history of TS, was found a pulsatile abdominal mass during the endocrinologist review for premature thelarche. On admission her height was 91cm, body weight 12kg, heart rate 130 bpm, body temperature 36.7ºC and blood pressure 94/63. Blood examination did not reveal any abnormalities. The brain magnetic resonance demonstrated calcified intracranial lesions (Figure 1). Cardiac evaluation revealed a myocardial mass in the papillary muscle (Rhabdomyoma). Abdominal computed tomography showed a big infrarenal saccular aneurysm measuring 68,1 x 52,5 x 54,6 mm (Figure 2). The aortic bifurcation was not involved.
Surgical intervention was performed through a midline laparotomy revealing a 50 mm infrarenal aneurysm (Figure 3). With 1mg/kg IV heparin the girl underwent surgery consisting of infrarenal aorta aortic interposition of a 14mm Dacron tube graft (Figure 4), the rest of the abdominal aorta and the aortic bifurcation were left with normal diameters (7-8 mm). No complications were reported during the procedure. Her postoperative course was uneventful, and the patient was discharged on the fifth day. The girl recovered rapidly and returned to normal life. Anti-platelet therapy was used after AAA repair because of the large size of the graft. Histological examination of the excised aortic wall revealed fibrosis and calcification. Frequent follow-ups with ultrasounds showed no alterations.
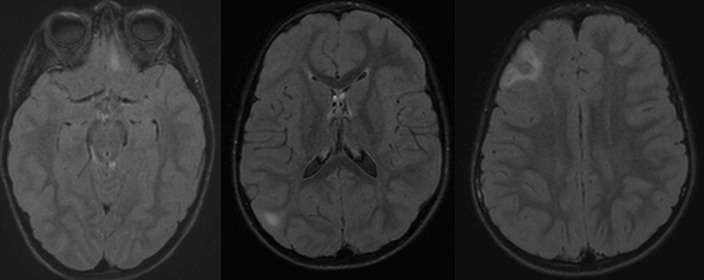
Figure 1: Brain MR. Calcific lesion in the right frontal lobe.

Figure 2: Angio CT. 3D Volume rendered image demonstrate an infrarenal aneurysm.
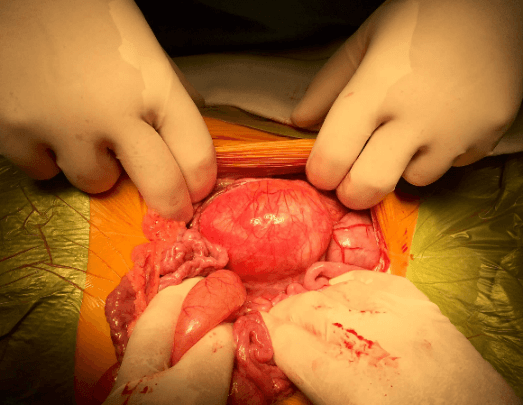
Figure 3: Surgical findings 50mm abdominal aortic aneurysm.
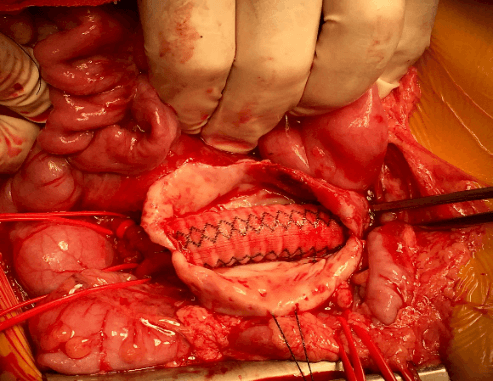
Figure 4: Infrarenal aorta aortic interposition of a 14mm Dacron tube graft.
Discussion
Tuberous sclerosis complex is a genetic disorder with autosomal-dominant inheritance; it is common in children. A variety of organs is frequently affected. The association between TS and aortic aneurysms is rarely observed, however, when presented it can be potentially risky. Aortic aneurysms in patients with TS are frequently missed, the diagnosis is usually incidental or after aneurysm rupture.
Open repair with interposition of an aorta aortic graft is the most direct surgical approach to treat this condition. In children, it is recommended the largest possible graft to allow proper vascular growth. Oversizing graft is one of the most important techniques [4-8]. Anticoagulation or anti-platelet therapy is difficult to conclude if it is necessary to use it, due to limited experience reported [3]. However, in our center based on our experience in adults’ cases undergoing Dacron vascular tube interposition surgery and Blalock-Taussig Shunt and Rastelli conduit surgeries in children, we propose following anti-platelet therapy for 1 year until the graft heals. Long-term follow-up is mandatory after this surgical intervention.
In conclusion, patients with TS should be screened for aortic disorders in order to rule out aortic aneurysms due to the high risk of rupture. This condition should be treated by early elective open repair surgery, performed in specialized center. Long-term follow-up is mandatory after surgical intervention.
Consent
The patient’s parents gave written permission for anonymous publication of patient data and medical images.
Article Info
Article Type
Case ReportPublication history
Received: Mon 27, Jul 2020Accepted: Fri 07, Aug 2020
Published: Sat 15, Aug 2020
Copyright
© 2023 José I. Aramendi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.08.19
Figures & Tables
References
- Peter B Crino, Katherine L Nathanson, Elizabeth Petri Henske (2006) The tuberous sclerosis complex. N Engl J Med 355: 1345-1356. [Crossref]
- Ann E Salerno, Olivera Marsenic, Kevin E C Meyers, Bernard S Kaplan, Jeffrey C Hellinger (2010) Vascular involvement in tuberous sclerosis. Pediatr Nephrol 25: 1555-1561. [Crossref]
- S B Moon, W Y Shin, Y J Park, S J Kim (2009) An abdominal aortic aneurysm in an 8-month-old girl with tuberous sclerosis. Eur J Vasc Endovasc Surg 37: 569-571. [Crossref]
- C J Jost, P Gloviczki, W D Edwards, A W Stanson, J W Joyce et al. (2001) Aortic aneurysms in children and young adults with tuberous sclerosis: report of two cases and review of the literature. J Vasc Surg 33: 639-642. [Crossref]
- Philip Dueppers, Mansur Duran, Klaus Grabitz, Hubert Schelzig (2017) Open Repair for Abdominal Aortic Aneurysm in a Young Boy with Tuberous Sclerosis and Review of the Literature. Ann Vasc Surg 39: 286.e1-286.e5. [Crossref]
- Andreas M E Koch, Rolf Janka, Werner Lang, Sven Dittrich (2008) Arterial aneurysm in tuberous sclerosis. Eur Heart J 29: 1282. [Crossref]
- Elie B Sawan, Roland Henaine, Linda Daou, Victor Jebara (2015) Successful Operation for Thoracoabdominal Aortic Aneurysm in a 5-Year-Old Boy With Tuberous Sclerosis. Ann Thorac Surg 100: e119-e120. [Crossref]
- Jonathan L Eliason, Dawn M Coleman, Enrique Criado, James C Stanley (2016) Surgical treatment of abdominal aortic aneurysms in infancy and early childhood. J Vasc Surg 64: 1252-1261. [Crossref]