Salvage Endoscopic Full-Thickness Resection of Colorectal Carcinoma after Radiotherapy in a Patient Not Eligible for Surgery
A B S T R A C T
For early, superficial colorectal carcinoma, endoscopic resection is an accepted curative treatment with an excellent long-term prognosis. Our report is the first report describing endoscopic full-thickness resection (eFTR) of residual recto-sigmoid carcinoma after radiotherapy. Our patient with cT2N0M0 recto-sigmoid carcinoma had been treated with radiotherapy because severe comorbidity precluded surgical resection. When the residual tumor was observed endoscopically, complete remission was achieved by endoscopic full thickness resection. There were no endoscopic or radiological signs of recurrent malignancy after the two-years follow-up period. In selected cases, eFTR after radiotherapy could be a curative treatment option.
Keywords
Colorectal carcinoma, endoscopic full-thickness resection, neoadjuvant radiotherapy, chemo-radiotherapy
Introduction
Colorectal carcinoma (CRC) is the third most commonly diagnosed type of malignancy in males, the second most common malignancy in females and the fourth leading cause of cancer-related deaths worldwide [1]. The cornerstone of curative therapy for colorectal carcinoma is surgical resection. For advanced colorectal carcinoma, the preferred curative treatment is neoadjuvant (chemo)radiotherapy (CRT) followed by surgical resection [2]. However, comorbidity does not always allow surgical intervention. In patients who are unfit for surgery, definitive CRT is an alternative, but local failure after definitive CRT at the primary site remains a significant problem. Two endoscopic techniques became available for the treatment of early-stage colorectal carcinoma in the last years: endoscopic submucosal dissection (ESD) and endoscopic full thickness resection (eFTR) [3]. We present a case where a patient with recto-sigmoid carcinoma who was not eligible for surgical intervention due to severe comorbidity. Initially, the carcinoma was not suitable for endoscopic resection as well. Finally, curation was reached by a salvage eFTR of residual tumor five months after (neo-adjuvant) radiotherapy with 5 Gray 5 times. The patient achieved long-term sustained remission.
Case Presentation
An 81-year-old male patient with a medical history of coronary-artery-bypass-grafting, bioprosthetic aortic-valve-replacement, DDD-R pacemaker implantation and severe chronic obstructive pulmonary disease was admitted to our hospital because of a prosthetic valve endocarditis due to Enterococcus faecalis. The endocarditis was treated with long course of antibiotics. Because of the Enterococcus faecalis bacteremia colonoscopy was performed. As the potential cause of the bacteremia a recto-sigmoid tumor 30 mm × 15 mm was noted (Figure 1) on endoscopy, and radiology suspected T2-carcinoma. Biopsies were performed and the diagnosis of adenocarcinoma was confirmed. CT-scan showed no signs of lymph node invasion or metastasis. Because of his comorbidities, the patient was not eligible for primary surgical resection. Endoscopic resection was not achievable due to suspicion of T2-carcinoma. After improvement of his clinical condition, 5 times 5 Gray local radiotherapy was provided.
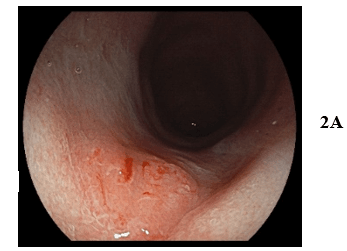
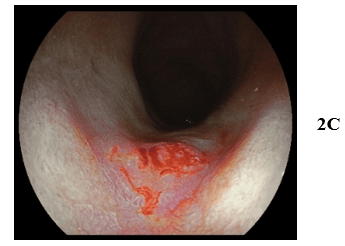
Three months after radiotherapy, sigmoidoscopy revealed a residual Paris type IIa lesion of 10 mm with Kudo Vi pit-pattern (Figure 2). The biopsies showed adenocarcinoma. Considering his comorbidities, surgical sigmoid resection was still not feasible. After a multidisciplinary discussion, we decided to perform an eFTR of the residual recto-sigmoid carcinoma. eFTR was scheduled five months after finishing radiotherapy. The residual carcinoma was completely removed (Figure 3). Histopathological analysis of the eFTR specimen showed well-/moderately differentiated adenocarcinoma with invasion in the submucosa (pT1) (Figure 4). Lymphangioinvasion and tumor budding was absent, and there were no poorly differentiated clusters. Resection margins were 0.4 cm free of carcinoma. No complications occurred during and after the procedure. In the next two years, colonoscopy (with biopsies of the scar) and CT-scan were performed every 6 months. Till now, there has been no sign of recurrent malignancy (Figure 5).
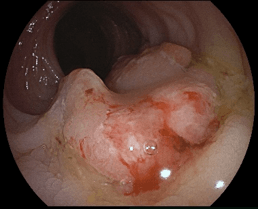
Figure 1: Initial colonoscopy showed a recto-sigmoid carcinoma; tension folds in the left side of the tumor during insufflation suggest ingrowth in the muscle layer.
Figure 2A, B & C: White Light, Blue Laser (BLI) and Linked Color Imaging (LCI) showed a residual Paris type IIa lesion of 10 mm with Kudo Vi pit-pattern.
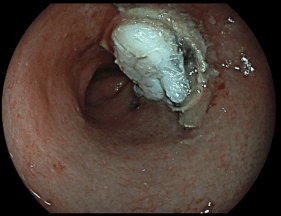
Figure 3: After eFTR the clip is in the right position, residual tumor is absent, and all colon layers are visible.
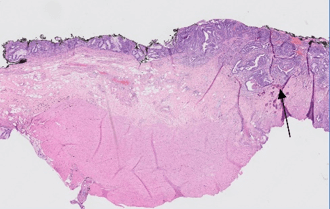
Figure 4: Full-thickness resection containing a well- to moderately differentiated adenocarcinoma with invasion in the submucosa (arrow). The stroma surrounding the tumor is partly fibrotic, with some calcifications. There is no tumor present in the underlying muscularis propria.
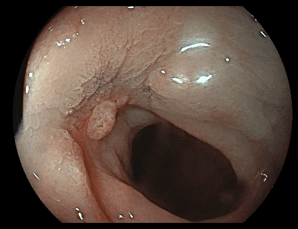
Figure 5: Colonoscopy 6 months after eFTR showed the scar with formation of granulation tissue in the center (histopathological confirmed).
Discussion
This is the first report of an endoscopic salvage eFTR of residual adenocarcinoma after (neo-adjuvant) radiotherapy. Our patient with an initial cT2N0M0 adenocarcinoma of the recto-sigmoid was treated with radiotherapy. Due to severe comorbidities, he was not eligible for surgical intervention. Complete remission could be achieved by salvage eFTR of the residual tumor. Sustained clinical remission was achieved. Endoscopic treatment was uncomplicated.
State-of-the-art treatment in the Netherlands for a T2 recto-sigmoid carcinoma is a low anterior resection. In the case of a locally advanced recto-sigmoid carcinoma, neoadjuvant treatment (radiotherapy or chemo-radiotherapy) followed by a subsequent resection is the preferred treatment [2]. Definitive (chemo) radiotherapy is regarded as the first-choice treatment for patients unfit for surgery. On the other hand, observation (watchful waiting strategy) with periodic colonoscopy is more common in patients who receive neo-adjuvant CRT with initially complete response [4]. Although CRT has shown a high response rate, local failure with recurrence or residual tumor is still common. In these cases, salvage endoscopic resection could be a curative treatment in selected patients. Endoscopic full-thickness resection has become the treatment of choice for small T1 carcinoma in the colon or rectum [5-7]. In the case of fibrosis, extra careful and patient maneuvering of the specimen into the eFTR cap must be performed.
For patients who are unfit for surgery but fit enough for systematic sedated endoscopy, long-term follow-up after CRT could be considered. Local control can be achieved by means of salvage endoscopic resection of small remnant or recurrent tumours in the absence of lymph node metastases. However, salvage endoscopic resection may be hampered by the development of submucosal fibrosis and the destruction of the colon wall layers after CRT.
Conclusion
Our report is the first report demonstrating that salvage eFTR of residual recto-sigmoid carcinoma after (neo-adjuvant) radiotherapy is feasible and a novel potential curative treatment in selected patients who are unfit for surgery.
Abbreviation
eFTR: endoscopic full-thickness resection
CRC: colorectal carcinoma
CRT: chemo-radiotherapy
RT: radiotherapy
ESD: endoscopic submucosal dissection
Article Info
Article Type
Case ReportPublication history
Received: Thu 09, Jan 2020Accepted: Fri 24, Jan 2020
Published: Fri 31, Jan 2020
Copyright
© 2023 Ramon-Michel Schreuder. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.01.12
Figures & Tables

References
- Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A et al. (2017) Global patterns and trends in colorectal cancer incidence and mortality. Gut 66: 683-691. [Crossref]
- Chen C, Sun P, Rong J, Weng HW, Dai QS et al. (2015) Short Course Radiation in the Treatment of Localized Rectal cancer: A Systematic Review and Meta-Analysis. Sci Rep 5: 10953. [Crossref]
- Aslanian HR, Sethi A, Bhutani MS, Goodman AJ, Krishnan K et al. (2019) ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection. VideoGIE 4: 343-350. [Crossref]
- Hassan C, Wysocki PT, Fuccio L, Seufferlein T, Dinis Ribeiro M et al. (2019) Endoscopic surveillance after surgical or endoscopic resection for colorectal cancer: European Society of Gastrointestinal Endoscopy (ESGE) and European Society of Digestive Oncology (ESDO) Guideline. Endoscopy 51: 266-277. [Crossref]
- van der Spek B, Haasnoot K, Meischl C, Heine D (2018) Endoscopic full-thickness resection in the colorectum: a single-center case series evaluating indication, efficacy and safety. Endosc Int Open 6: E1227-E1234. [Crossref]
- Andrisani G, Soriani P, Manno M, Pizzicannella M, Pugliese F et al. (2019) Colo-rectal endoscopic full-thickness resection (EFTR) with the over-the-scope device (FTRD®): A multicenter Italian experience. Dig Liver Dis 51: 375-381. [Crossref]
- Kuellmer A, Mueller J, Caca K, Aepli P, Albers D et al. (2019) Endoscopic full-thickness resection for early colorectal cancer. Gastrointest Endosc 89: 1180-1189. [Crossref]