Clinicopathologic Characteristics and Treatment Outcomes of Rectal Gastrointestinal Stromal Tumors: A Retrospective Study
A B S T R A C T
Background and Study Aims: To investigate the clinicopathologic characteristics, surgical and imatinib management and long-term follow-up outcomes of the rectal gastrointestinal stromal tumors (GISTs).
Patients and Methods: Consecutive patients with rectal GISTs admitted to our center (from January 2013 to June 2018) were chosen. Their history information was viewed, and the follow-up results were obtained by phone or medical records.
Results: Forty-nine patients (32 males and 17 females) were identified, with a median age of 59 years, and 36 patients received surgery. Most (46 patients, 93.9%) of the tumor were located within 6 cm from the anal verge, 18 patients (36.7%) had very low or low risk, and 31 patients (63.3%) had intermediate or high risk. Four kinds of surgery approach were applied in our center: trans-abdominal (8 patients, 22.2%), trans-anal/trans-perineal (15 patients, 41.7%), trans-sacral (12 patients, 33.3%) and abdominoperineal (1 patient, 2.8%). The complication is low and the mortality related to surgery is 0%. After a median follow-up of 705 days (ranged from 48 days to 1677 days), 3 patients (8.33%) were found to have a recurrence.
Conclusion: Trans-anal/trans-perineal and trans-sacral surgery were more commonly used in our study, and for now, the recurrence rate had no difference, but a longer time for follow-up is needed.
Keywords
GIST, rectal, surgery, recurrence
Introduction
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors of the gastrointestinal tract [1]. GISTs can originate from any part of the gastrointestinal tract, with the highest frequency in the stomach and small intestine, while it is relatively rare in the rectum, which accounts for approximately 5% of all GISTs [2]. Complete resection of the tumor is the cornerstone of treatment of localized GISTs, but it is difficult in the rectum due to its anatomical features associated with the pelvis, sphincter muscle and other organs [3]. Till now, no guidelines or consensus has highlighted the optimum surgical approach, and surgeons select the surgical procedure mainly based on the tumor location and size. Furthermore, therapy with imatinib is reported to be highly effective in reducing the sizes of advanced GISTs, increasing the anas-preserving rate, and improving both surgical and survival outcomes [4-7]. The experience of rectal GISTs treatment is limited in the literature up to now, and most studies are small sample-sized, so we conducted this study to share our experience in rectal GISTs from the aspects of clinicopathologic characteristics, surgical and imatinib management and long-term follow-up outcomes [1, 8]. We present the following article in accordance with the STROBE (Link) reporting checklist.
Materials and Methods
I Patients and Data Collection
From January 2013 to June 2018, consecutive patients with rectal GISTs admitted to our center were retrospectively reviewed. Patients were included if their specimens of needle aspiration tissues or surgical tissues were pathologically proven to be rectal GISTs. Patients were excluded if they met any of the following criteria: a) the GISTs located in any other part of the gastrointestinal tract except in the rectum; b) foreign patients. Patients’ history information, laboratory tests, endoscopic results, ultrasonography results, computed tomography (CT) or magnetic resonance imaging (MRI) results, surgery procedure details and status after the surgery were viewed. Then we obtained the follow-up results by telephoning the patients or by searching for the medical records in our hospital since this hospitalization. The study protocol was approved by the institutional review board.
II Statistical Analysis
All statistical analysis was performed by IBM SPSS Statistic Version 24.0.0.0. Continuous variables with normal distribution were expressed with mean and standard deviation (SD). Continuous variables without normal distribution were expressed with median and range. Categorical variables were expressed with numbers and percentages. Kaplan-Meier survival analysis was used to assess the recurrence-free survival of the patients who underwent surgery.
Results
I Patient Characteristics
We finally identified 49 patients (32 males and 17 females), with a median age of 59 years, and among which 36 patients received surgery, while 13 patients did not. Upon diagnosis, 2 patients (4.1%) were found to have liver metastasis. Nine patients have been diagnosed with rectal GISTs, and received surgery before, and diagnosed with recurrence this time. The top five common chief complaints were rectal pain or discomfort (21 patients, 42.9%), change of bowel habits (20 patients, 40.8%), rectal bleeding (16 patients, 32.7%), difficult defecation (14 patients, 28.6%), and discovered by health examination without any symptoms (17 patients, 34.7%). The size of the tumor ranged from 0.5 cm to 14.7 cm, with a median of 5 cm. Most (46 patients, 93.9%) of the tumor were located within 6 cm from the anal verge (Table 1). Based on the National Institute of Health (NIH) risk categories, 18 patients (36.7%) had very low or low risk, and 31 patients (63.3%) had intermediate or high risk. Seven patients had KIT mutation detection, 6 patients had a mutation in KIT exon 11, and one patient had a mutation in KIT exon 9. Six patients also had platelet derived growth factor receptor α (PDGFRA) mutation detection, and 3 patients had a mutation in PDGFRA exon 18, and 3 patients with wild type. The immunohistochemical results of the tumors are shown in (Table 2).
Table 1: The demographic characteristics of the patients with rectal
gastrointestinal stromal tumors.
|
Contents |
Number |
Percentage (%) |
|
Age (years) |
|
|
|
<60 |
29 |
59.2 |
|
≥60 |
20 |
40.8 |
|
Gender |
|
|
|
Male |
32 |
65.3 |
|
Female |
17 |
34.7 |
|
Symptoms * |
|
|
|
No symptoms |
17 |
34.7 |
|
Rectal bleeding |
16 |
32.7 |
|
Rectal pain or discomfort |
21 |
42.9 |
|
Difficult defecation |
14 |
28.6 |
|
Change of bowel habits |
20 |
40.8 |
|
Mass protruded |
2 |
4.1 |
|
Urinary Symptoms |
3 |
6.1 |
|
Tumor size (cm) |
|
|
|
<5 |
24 |
49.0 |
|
≥5 |
25 |
51.0 |
|
Distance from anal verge (cm) |
|
|
|
<6 |
46 |
93.9 |
|
≥6 |
3 |
6.1 |
|
NIH risk categories |
|
|
|
Very low and low |
18 |
36.7 |
|
Intermediate and high |
31 |
63.3 |
|
Tumor rupture |
1 |
2.0 |
|
Recurrent patients |
9 |
18.4 |
|
Liver metastasis |
2 |
4.1 |
|
Follow-up time (days) |
705 (48-1677) |
|
*Some patients have more than one
symptom. NIH: National Institute of Health.
Table 2: The immunohistochemical results of the patients with rectal GIST.
|
Immunohistochemistry |
Positive rate |
|
CD117 |
97.8%(45/46) |
|
CD34 |
97.8%(45/46) |
|
DOG-1 |
97.7%(42/43) |
|
Desmin |
4.7%(2/43) |
|
Actin |
9.5%(4/42) |
|
S-100 |
14.0%(6/43) |
|
Ki-67 |
92.9%(39/42) |
II Imatinib Mesylate Treatment and Surgery
For 13 patients, the sizes of the tumor were very large and the tumor invaded other organs in the pelvis. After multidisciplinary consultation, imatinib mesylate was advised. The other 36 patients received surgery, and among whom 15 patients had received imatinib treatment before surgery and based on the NIH risk categories and patients’ economic status, 16 patients received imatinib treatment after surgery. In summary, there were four kinds of surgical procedures, including trans-abdominal (8 patients, 22.2%), trans-anal/trans-perineal (15 patients, 41.7%), trans-sacral (12 patients, 33.3%) and abdominoperineal (1 patient, 2.8%). The background patterns of the tumors in each group are shown in (Table 3). The most common complications after surgery were fistula (5 patients, 13.9%), including anastomotic fistula (2 patients, 5.6%), rectal skin fistula (1 patient, 2.8%), rectovaginal fistula (2 patients, 5.6%). Other complications were abdominal/pelvis infection (3 patients, 8.3%), wound infection (1 patient, 2.8%), disruption of wound (1 patient, 2.8%) and pelvic floor hernia (1 patient, 2.8%). All patients recovered from the operative or/ and conservative treatment, and the mortality related to surgery is 0%. The median hospital stay was 23.5 days for the patients receiving surgery, with a range from 3 days to 90 days.
Table 3: Background patterns and surgical outcomes of different surgical
procedures.
|
Item |
Trans-abdominal |
Trans-anal/trans-perineal |
Trans-sacral |
Abdominoperineal |
|
Patients |
8 |
15 |
12 |
1 |
|
Sex (F:M) |
1:7 |
7:8 |
4:8 |
1:0 |
|
Tumor size (cm) |
|
|
|
|
|
<5 |
4 |
11 |
7 |
0 |
|
≥5 |
4 |
4 |
5 |
1 |
|
Distance from anal verge |
|
|
|
|
|
<6 cm |
8 |
15 |
11 |
1 |
|
≥6 cm |
0 |
0 |
1 |
0 |
|
NIH risk categories |
|
|
|
|
|
Very low and low (%) |
3 (37.5) |
9 (60.0) |
4 (33.3) |
0 (0.0) |
|
Intermediate and high (%) |
5 (62.5) |
6 (40.0) |
8 (66.7) |
1 (100.0) |
|
Sphincter preservation (%) |
6 (75.0) |
15 (100.0) |
11 (100.0) |
0 (0.0) |
|
Complications |
|
|
|
|
|
Pelvic floor hernia (%) |
1 (12.5) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Abdominal/pelvic infection (%) |
2 (25) |
0 (0.0) |
1 (8.3) |
0 (0.0) |
|
Wound infection (%) |
1 (12.5) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Disruption of Wound (%) |
0 (0.0) |
0 (0.0) |
1 (8.3) |
0 (0.0) |
|
Fistula (%) |
0 (0.0) |
3 (20.0) |
2 (16.7) |
0 (0.0) |
|
Hospital Stay (days) |
31.5 (18-90) |
19 (3-37) |
28 (16-60) |
43 |
|
Recurrent patients (%) |
1 (12.5) |
2 (13.3) |
0 (0.0) |
0 (0.0) |
III Follow-up Results
After a median follow-up of 705 days (ranged from 48 days to 1677 days), for the 36 patients who received surgery, 2 patients (5.56%) got lost, 3 patients (8.33%) were found to have a recurrence. Figure 1 shows the recurrence-free survival (RFS) curves of the patients who received surgery. And for the 13 patients who did not receive surgery but received imatinib, 2 patients (15.38%) were lost during follow-up, 2 patients (15.38%) had advancement, 8 patients (61.54%) had regression, and 1 patient stayed the same.
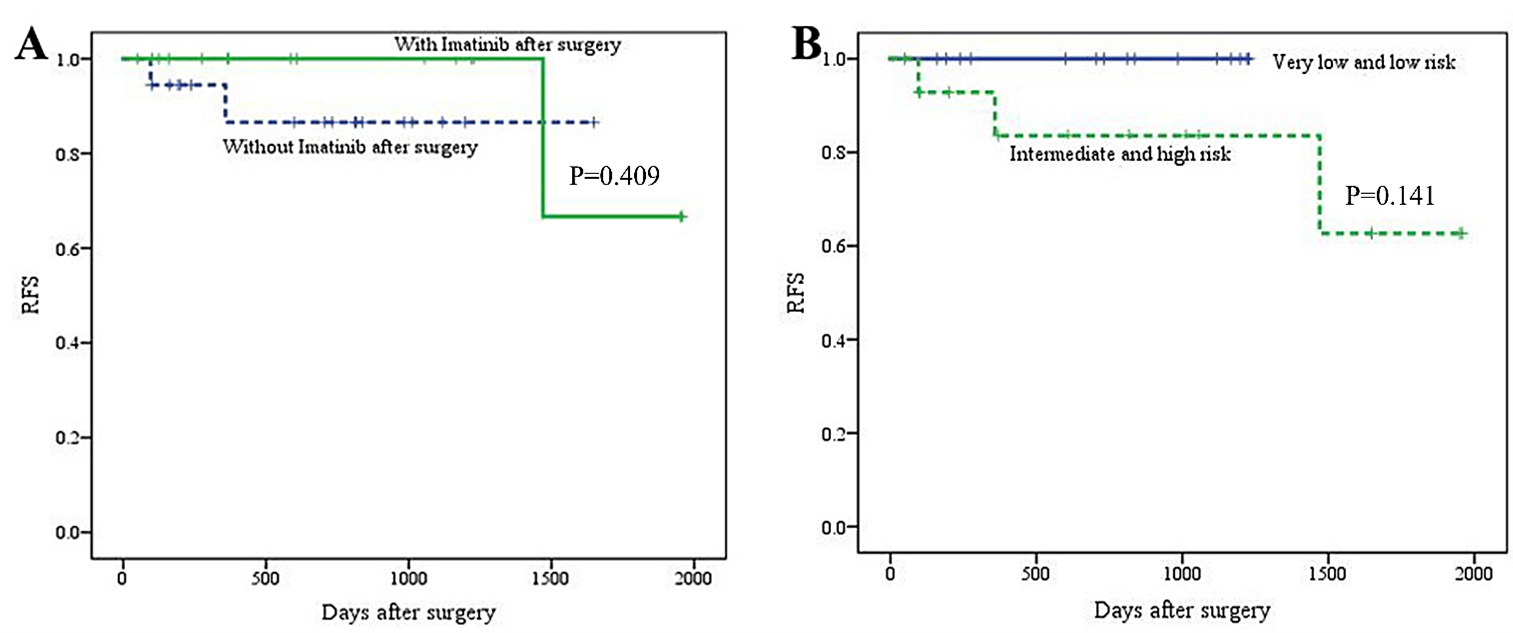
Figure 1: Recurrence-free survival (RFS) curves of A) the patients who received VS. did not receive imatinib after the surgery, B) the patients with very low and low risk VS. intermediate and high risk.
Discussion
Rectal GISTs are much less common compared to GISTs in the stomach and small intestine, and their clinical features and treatment outcomes were not well documented. In this study, we analysed the clinicopathologic characteristics, surgery approach, the usage of imatinib and follow-up outcomes of rectal GISTs. In this study, the patients’ median age was 59 years, and 65.3% of those were male. Most (46 patients, 93.9%) of the tumor were located within 6 cm from the anal verge with a median of 5 cm, consistent with previous reports [9-11]. Because it is easy to occur in the middle and lower part of the rectum, a digital rectal examination is a very important way to find lesions. It can roughly judge its position, shape, hardness, tenderness, mobility and observe whether the fingertip is stained with blood when withdrawing. The main primary symptoms were anal discomfort or pain, bleeding, constipation and others [12, 13]. Gastrointestinal endoscopy, contrast-enhanced CT and MRI are the common diagnostic methods, and transrectal ultrasound-guided biopsy can diagnose the stromal tumor and guide the treatment [14].
The stromal tumors are mainly composed of spindle cells, but they need to be differentiated from leiomyomas and leiomyosarcomas [15]. The immunohistochemical analysis can be CD117 (KIT) positive dominantly, CD34, PDGFRA, smooth muscle actin, S-100, and vimentin-positive occasionally. Miettinen et al. reported that the expression rates of CD117 and CD34 in 96 cases of rectal GISTs were 100% and 94%, respectively [16]. In this study, the expression rates of CD117 and CD34 were 97.8% and 97.8% in sequence, which was similar to the previous literature. KIT mutation detection is reported to be similar to that of the small intestinal stromal tumor, and KIT exon 11 mutation is the most common, while PDGFRA mutation rarely occurs in rectal GISTs [17].
Previous studies have suggested that patients with high risk were more likely to have distant metastasis, while patients with low risk were more likely to have a local recurrence. In this study, the recurrence rate and metastasis rate were not statistically significant in the two groups. The reason for this might be the sample size was not large enough and the time for follow-up was relatively not long enough. Landi et al. described that patients with local resection had a higher postoperative recurrence rate, while in this study, patients with anal resection accounted for only 13.3%, and patients with anal operation had the shortest hospitalization time [18]. Because of the special anatomical structure, different surgical methods are directly related to the quality of the patients' life after operation [19]. Although the incidence of anal fistula was the highest, it seemed to be the first choice for rectal stromal tumors less than 5 cm.
Imatinib can selectively inhibit the growth of stromal tumors by blocking the c-Kit-mediated signal pathway [20]. The partial remission rate of the inoperable stromal tumor can reach 40% [21]. In this study, the remission rate of the inoperable rectal stromal tumor after taking imatinib was 61.5% (8/13). Fujimoto et al. reported that imatinib could prolong the survival period and improve the rate of anus preservation [22]. In this study, 15 patients who used imatinib before the operation were all succeeded in anus preservation, and the rate of anus preservation without using imatinib was 85.7% (18/21). Postoperative adjuvant treatment is determined according to the risk of malignancy [4, 5]. The risk of rectal stromal tumor is high, but the clinical experience is not enough. It is necessary to make clear its clinical characteristics, development and outcome, apply individualized treatment plans to patients, and make close follow-ups after the operation. However, how to improve the diagnosis rate before the operation, how to choose the operation method, how to determine the dose and time limit of imatinib treatment in the perioperative period are still controversial, and multi-centered prospective research is urgently needed.
Conclusion
Rectal GISTs are becoming increasingly common, and complete resection of the tumor is the cornerstone of the treatment of localized GISTs. In our study, most of the tumors were localized within 6 cm from the anal verge, so trans-anal/trans-perineal and trans-sacral surgery were more common and safe, the recurrence rate had no difference in each group for now, but a longer time for follow-up is still needed.
Conflicts of Interest
None.
Article Info
Article Type
Research ArticlePublication history
Received: Tue 20, Apr 2021Accepted: Tue 04, May 2021
Published: Mon 31, May 2021
Copyright
© 2023 Chujun Li. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.05.04
Figures & Tables
Table 1: The demographic characteristics of the patients with rectal
gastrointestinal stromal tumors.
|
Contents |
Number |
Percentage (%) |
|
Age (years) |
|
|
|
<60 |
29 |
59.2 |
|
≥60 |
20 |
40.8 |
|
Gender |
|
|
|
Male |
32 |
65.3 |
|
Female |
17 |
34.7 |
|
Symptoms * |
|
|
|
No symptoms |
17 |
34.7 |
|
Rectal bleeding |
16 |
32.7 |
|
Rectal pain or discomfort |
21 |
42.9 |
|
Difficult defecation |
14 |
28.6 |
|
Change of bowel habits |
20 |
40.8 |
|
Mass protruded |
2 |
4.1 |
|
Urinary Symptoms |
3 |
6.1 |
|
Tumor size (cm) |
|
|
|
<5 |
24 |
49.0 |
|
≥5 |
25 |
51.0 |
|
Distance from anal verge (cm) |
|
|
|
<6 |
46 |
93.9 |
|
≥6 |
3 |
6.1 |
|
NIH risk categories |
|
|
|
Very low and low |
18 |
36.7 |
|
Intermediate and high |
31 |
63.3 |
|
Tumor rupture |
1 |
2.0 |
|
Recurrent patients |
9 |
18.4 |
|
Liver metastasis |
2 |
4.1 |
|
Follow-up time (days) |
705 (48-1677) |
|
*Some patients have more than one
symptom. NIH: National Institute of Health.
Table 2: The immunohistochemical results of the patients with rectal GIST.
|
Immunohistochemistry |
Positive rate |
|
CD117 |
97.8%(45/46) |
|
CD34 |
97.8%(45/46) |
|
DOG-1 |
97.7%(42/43) |
|
Desmin |
4.7%(2/43) |
|
Actin |
9.5%(4/42) |
|
S-100 |
14.0%(6/43) |
|
Ki-67 |
92.9%(39/42) |
Table 3: Background patterns and surgical outcomes of different surgical
procedures.
|
Item |
Trans-abdominal |
Trans-anal/trans-perineal |
Trans-sacral |
Abdominoperineal |
|
Patients |
8 |
15 |
12 |
1 |
|
Sex (F:M) |
1:7 |
7:8 |
4:8 |
1:0 |
|
Tumor size (cm) |
|
|
|
|
|
<5 |
4 |
11 |
7 |
0 |
|
≥5 |
4 |
4 |
5 |
1 |
|
Distance from anal verge |
|
|
|
|
|
<6 cm |
8 |
15 |
11 |
1 |
|
≥6 cm |
0 |
0 |
1 |
0 |
|
NIH risk categories |
|
|
|
|
|
Very low and low (%) |
3 (37.5) |
9 (60.0) |
4 (33.3) |
0 (0.0) |
|
Intermediate and high (%) |
5 (62.5) |
6 (40.0) |
8 (66.7) |
1 (100.0) |
|
Sphincter preservation (%) |
6 (75.0) |
15 (100.0) |
11 (100.0) |
0 (0.0) |
|
Complications |
|
|
|
|
|
Pelvic floor hernia (%) |
1 (12.5) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Abdominal/pelvic infection (%) |
2 (25) |
0 (0.0) |
1 (8.3) |
0 (0.0) |
|
Wound infection (%) |
1 (12.5) |
0 (0.0) |
0 (0.0) |
0 (0.0) |
|
Disruption of Wound (%) |
0 (0.0) |
0 (0.0) |
1 (8.3) |
0 (0.0) |
|
Fistula (%) |
0 (0.0) |
3 (20.0) |
2 (16.7) |
0 (0.0) |
|
Hospital Stay (days) |
31.5 (18-90) |
19 (3-37) |
28 (16-60) |
43 |
|
Recurrent patients (%) |
1 (12.5) |
2 (13.3) |
0 (0.0) |
0 (0.0) |
References
1.
Tielen R, Verhoef
C, van Coevorden F, Reyners AK, van der Graaf WTA et al. (2013) Surgical
management of rectal gastrointestinal stromal tumors. J Surg Oncol 107:
320-323. [Crossref]
2.
Tran T, Davila JA,
El Serag HB (2005) The epidemiology of malignant gastrointestinal stromal
tumors: an analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol
100: 162-168. [Crossref]
3.
Kameyama H, Kanda
T, Tajima Y, Shimada Y, Ichikawa H et al. (2018) Management of rectal
gastrointestinal stromal tumor. Transl Gastroenterol Hepatol 3: 8. [Crossref]
4.
Dematteo RP,
Ballman KV, Antonescu CR, Maki RG, Pisters PWT et al. (2009) Adjuvant imatinib
mesylate after resection of localised, primary gastrointestinal stromal tumour:
a randomised, double-blind, placebo-controlled trial. Lancet 373:
1097-1104. [Crossref]
5.
Joensuu H,
Eriksson M, Sundby Hall K, Hartmann JT, Pink D et al. (2012) One vs three years
of adjuvant imatinib for operable gastrointestinal stromal tumor: a randomized
trial. JAMA 307: 1265-1272. [Crossref]
6.
Baik SH, Kim NK,
Lee CH, Lee KY, Sohn SK et al. (2007) Gastrointestinal stromal tumor of the
rectum: an analysis of seven cases. Surg Today 37: 455-459. [Crossref]
7.
Jakob J, Mussi C,
Ronellenfitsch U, Wardelmann E, Negri T et al. (2013) Gastrointestinal stromal
tumor of the rectum: results of surgical and multimodality therapy in the era
of imatinib. Ann Surg Oncol 20: 586-592. [Crossref]
8.
Liu H, Yan Z,
Liao G, Yin H (2014) Treatment strategy of rectal gastrointestinal stromal
tumor (GIST). J Surg Oncol 109: 708-713. [Crossref]
9.
Rammohan A,
Sathyanesan J, Rajendran K, Pitchaimuthu A, Perumal SK et al. (2013) A gist of
gastrointestinal stromal tumors: A review. World J Gastrointest Oncol 5:
102-112. [Crossref]
10.
Kirsch R, Gao ZH,
Riddell R (2007) Gastrointestinal stromal tumors: diagnostic challenges and
practical approach to differential diagnosis. Adv Anat Pathol 14:
261-285. [Crossref]
11.
Hawkins AT, Wells
KO, Krishnamurty DM, Hunt SR, Mutch MG et al. (2017) Preoperative Chemotherapy
and Survival for Large Anorectal Gastrointestinal Stromal Tumors: A National
Analysis of 333 Cases. Ann Surg Oncol 24: 1195-1201. [Crossref]
12.
Pai VD, Demenezes
JL, Patil PS, Saklani AP (2016) Multimodality therapy of rectal
gastrointestinal stromal tumors in the era of imatinib-an Indian series. J
Gastrointest Oncol 7: 262-268. [Crossref]
13.
Shen C, Chen H,
Yin R, Yin Y, Chen J et al. (2015) Clinicopathologic, surgical characteristics
and survival outcomes of rectal gastrointestinal stromal tumors. Neoplasma
62: 610-617. [Crossref]
14.
Koo DH, Ryu MH,
Kim KM, Yang HK, Sawaki AK et al. (2016) Asian Consensus Guidelines for the
Diagnosis and Management of Gastrointestinal Stromal Tumor. Cancer Res Treat
48: 1155-1166. [Crossref]
15.
Zarkavelis G,
Petrakis D, Pavlidis N (2015) Gastrointestinal stromal tumors during pregnancy:
a systematic review of an uncommon but treatable malignancy. Clin Transl
Oncol 17: 757-762. [Crossref]
16.
Miettinen M, Furlong M, Sarlomo Rikala M, Burke A, Sobin
LH et al. (2001) Gastrointestinal stromal tumors, intramural
leiomyomas, and leiomyosarcomas in the rectum and anus: a clinicopathologic,
immunohistochemical, and molecular genetic study of 144 cases. Am J Surg
Pathol 25: 1121-1133. [Crossref]
17.
Miettinen M,
Lasota J (2005) KIT (CD117): a review on expression in normal and neoplastic
tissues, and mutations and their clinicopathologic correlation. Appl
Immunohistochem Mol Morphol 13: 205-220. [Crossref]
18.
Landi B, Bouche
O, Guimbaud R, Chayyvialle JA (2010) [Gastrointestinal stromal tumors
(GIST)<5 cm in size: review of the literature and expert propositions for
clinical management]. Gastroenterol Clin Biol 34: 120-133. [Crossref]
19.
Rosa F, Alfieri S, Tortorelli AP, Miceli DD, Papa V et
al. (2012) Gastrointestinal stromal tumors: prognostic factors and
therapeutic implications. Tumori 98: 351-356. [Crossref]
20.
Agaimy A, Bauer
S, Beham A, Bertolini J, Haller F et al. (2015) [Gastrointestinal stromal
tumours (GIST)--development in pathology, surgery and medical therapy.
Developed during the 10th German GIST-meeting, Göttingen]. Z Gastroenterol
53: 235-243. [Crossref]
21.
Li K, Cheng H, Li Z, Pang Y, Jia X et al. (2017) Genetic
progression in gastrointestinal stromal tumors: mechanisms and molecular
interventions. Oncotarget 8: 60589-60604. [Crossref]
22. Fujimoto Y, Akiyoshi
T, Konishi T, Nagayama S, Fukunaga Y et al. (2014) Laparoscopic
sphincter-preserving surgery (intersphincteric resection) after neoadjuvant
imatinib treatment for gastrointestinal stromal tumor (GIST) of the rectum. Int
J Colorectal Dis 29: 111-116. [Crossref]