Urgent Endovascular Treatment of Severe Celiac Artery Stenosis during Liver Transplantation
Urgent Endovascular Treatment of Severe Celiac Artery Stenosis during Liver Transplantation
A B S T R A C T
Arterial reconstruction during orthotopic liver transplant (OLT) can often be quite challenging in cases where the recipient hepatic artery is inadequate to provide inflow to the allograft. In these situations, an aorto-hepatic interposition graft is typically performed using the donor iliac artery [1, 2]. We present a case describing the use of urgent endovascular treatment of severe celiac artery stenosis intra-operatively during liver transplantation in a patient with significant aorto-iliac atherosclerotic disease precluding the use of an interposition graft.
Keywords
Liver transplantation, arterial reconstruction, endovascular revascularization, arterial inflow, hepatic reperfusion
Case Report
The patient is a 64-year-old female with end stage liver disease (ESLD) secondary to nonalcoholic steatohepatitis (NASH) cirrhosis along with hypertension, hyperlipidemia, and known peripheral arterial disease (PAD). Preoperative workup did reveal significant atherosclerotic disease. On pre-operative computed tomography angiography (CTA), she had evidence of celiac, superior mesenteric artery (SMA), and inferior mesenteric artery (IMA) stenosis along with severe narrowing of bilateral renal and iliac vessels. She did have an abdominal ultrasound with doppler that revealed patent main, right, and left hepatic arteries with peak systolic velocities of 144, 67, and 61cm/second respectively. This was reviewed by the selection committee and felt to be suitable for transplantation.
On March 18, 2019, the patient underwent an OLT using a whole liver from a Donor after Brain Death (DBD). Intra-operatively, both donor and recipient arterial anatomy were found to be standard. Graft arterial inflow was provided by anastomosing the donor common hepatic artery to the recipient right-left hepatic branch patch using 6-0 polypropylene suture. Following this, arterial inflow was assessed and noted to be extremely poor. An intra-operative ultrasound was obtained which revealed flow within the left hepatic artery but with tardus parvus waveforms and a resistive index (RI) of 0.35 indicating severe stenosis [3]. No flow was visualized within the main hepatic artery. At this point, we attempted to improve arterial inflow by passing a Fogarty catheter across the area of known celiac artery stenosis. There was some improvement in flow following this maneuver, but it was still felt to be inadequate. The recipient infra-renal aorta and iliac vessels were then examined for possible interposition graft using autogenous donor artery. Given pre-operative imaging findings of severe atherosclerotic disease in the recipient and heavily calcified arteries noted intra-operatively, we did not feel there was a safe area for cross clamping. Given the patient’s body habitus, it was too hazardous to attempt exposure of the supra-celiac aorta.
Vascular surgery was consulted at this time to assess for alternatives to improve arterial inflow. Decision was made to perform a selective celiac arteriogram with possible intervention. For this to be possible, the patient had to be transferred to our hybrid operating room. The patient was left in biliary discontinuity and an external biliary drain was placed. Her abdomen was left open and an Abthera VAC was placed. She was then transported to the hybrid operating room. A selective celiac arteriogram was performed revealing a focal high-grade celiac ostial stenosis of >80% (Figure 1). This area was balloon dilated followed by placement of a 6x15mm Herculink balloon expandable drug eluding stent. A completion angiogram was then performed showing <20% residual celiac stenosis (Figure 2). The patient was kept intubated and transported to the surgical intensive care unit with plans to return to the operating room within 24 hours.
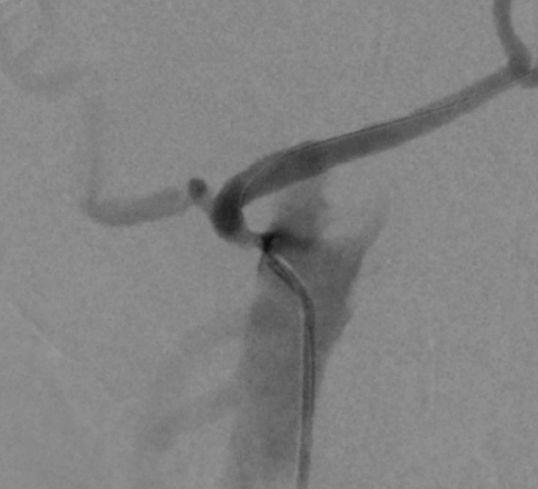
Figure 1: Selective celiac arteriogram showing focal high-grade ostial stenosis.

Figure 2: Arteriogram status post celiac artery stenting showing near resolution of stenosis.
The following day, she was taken back to the operating room and a good pulse was noted within the main hepatic artery which had not been present prior to the celiac stent placement. The biliary anastomosis was created, and the transplant was completed. An ultrasound was obtained the following day that demonstrated a patent celiac artery and hepatic arterial system. Main hepatic artery peak systolic velocity was measured at 273cm/sec with an RI of 0.57 and normal waveforms. The remainder of the patient’s postoperative course was relatively uncomplicated. She was started on dual antiplatelet therapy with Aspirin and Clopidogrel. She was discharged to rehab on post-op day 10. Abdominal ultrasound performed at two months and one-year post-transplant revealed a patent hepatic arterial system with RIs within the normal range and normal waveforms.
Discussion
Although the use of endovascular techniques to treat arterial complications following liver transplantation is widely described in the literature, we describe here a unique situation where it was used intra-operatively to provide arterial inflow. Even with evidence of significant aorto-iliac calcifications on pre-operative CTA, we opted to proceed with OLT given the encouraging doppler ultrasound findings. However, by identifying the clinically significant celiac stenosis intra-operatively, we were able to immediately intervene on it to prevent prolonged arterial ischaemia to the allograft and the resultant biliary complications.
Abbreviations
OLT: Orthotopic Liver Transplant
ESLD: End Stage Liver Disease
NASH: Nonalcoholic Steatohepatitis
PAD: Peripheral Arterial Disease
CTA: Computed Tomography Angiography
SMA: Superior Mesenteric Artery
IMA: Inferior Mesenteric Artery
DBD: Donor After Brain Death
RI: Resistive Index
Article Info
Article Type
Case ReportPublication history
Received: Wed 21, Oct 2020Accepted: Mon 02, Nov 2020
Published: Thu 12, Nov 2020
Copyright
© 2023 Tung Vu. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.TCR.2020.02.05
Figures & Tables
References
- Jung DH, Park CS, Ha TY, Song GW, Park GC et al. (2018) Placement of an Aortohepatic Conduit as an Alternative to Standard Arterial Anastomosis in Liver Transplantation. Ann Transplant 23: 61-65. [Crossref]
- Denecke C, Weiss S, Biebl M, Fritz J, Dziodzio T et al. (2016) An Arterial Conduit Is Not a Risk Factor for Survival Following Orthotopic Liver Transplantation: An Analysis of 20 Years of Liver Transplantation in Innsbruck. Ann Transplant 21: 321-328. [Crossref]
- Criado AG, Gilabert R, Berzigotti A, Brú C (2009) Doppler Ultrasound Findings in the Hepatic Artery Shortly After Liver Transplantation. AJR Am J Roentgenol 193: 128-135. [Crossref]