Transient Sigmoidorectal Intussusception Simulating Submucosal Tumor in a Healthy Woman: An Unusual Case and Review of the Literature
A B S T R A C T
A 42-year-old healthy woman underwent scheduled polypectomy. The introduction of colonoscope showed a rectal regular subepithelial mass with an aperture on the top but the passage of the endoscope was impossible. By introducing gastroscope, however, the mass had disappeared. Subsequently, an uneventful colonoscopy was performed with resection of three small polyps located in ascending and transverse colon. Transient sigmoidorectal intussusception was the diagnosis, which is a very rare condition.
Keywords
Rectal submucosal tumor, adult intussusception, transient intussusception, case report, colonoscopy
Introduction
Intussusception is defined as the invagination of proximal segment of bowel into a peripheral distal segment. Adult intussusception is a rare clinical entity and accounts for less than 5% of all intussusception cases; it is a challenging condition, particularly when located in the colon; and it usually demands preoperative diagnostic skills, careful and attentive intra-operative decision, and suitable postoperative follow-up to anticipate a successful outcome [1-5].
The precise mechanism of origin of intussusception is still unidentified. It is assumed that any lesion in the gut wall or irritant within the lumen of the bowel that alters normal peristaltic activity is able to induce intussusception. Ingested food and consequent gut peristaltic activity create an area of constriction above the stimulus and relaxation below, thus telescoping the lead point across the lumen of the distal bowel [5]. Certain intussusceptions might resolve spontaneously without surgical intervention. Such intussusceptions are called transient.
We hereby describe a very rare case of transient sigmoidorectal intussusception simulating submucosal tumor in a healthy woman who underwent scheduled polypectomy.
Case Report
A fit and healthy 42-year-old woman, with no significant surgical and medical history underwent screening colonoscopy by a private gastroenterologist. She was found to have three small (<1cm) polyps in ascending and transverse colon. No other findings were reported, especially in rectal cavity. The introduction of colonoscope in rectal cavity showed a regular subepithelial mass with a central ulceration or aperture on the top (Figures 1A & 1B). A close view revealed to be aperture. We tried to pass the aperture, but it was impossible, because the diameter of opening was smaller to colonoscope’s diameter. By introducing a gastroscope surprisingly the mass had disappeared. In turn, an uneventful colonoscopy was performed with resection of three polyps. Our patient continues to be symptomatic one year later.
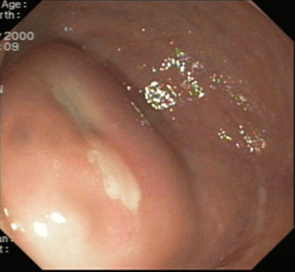
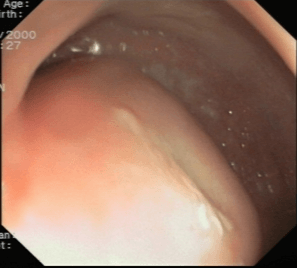
Figure 1:A) Endoscopic view of a submucosal mass with an aperture in the centrum. B) Another view of the mass.
Discussion
Intussusception in adults is rare, although being common in children; it accounts for 1% of patients having bowel obstruction, and 5–10% of all intussusception occasions; and approximately 90% of adults with intussusception have an underlying lesion, almost half of which are malignant [6]. Intussusception results from the change of normal peristalsis by a lesion in the gut wall that induces invagination; it is demarcated as the invagination of one segment of the bowel into an immediately adjacent segment. The intussusceptum denotes the proximal segment that invaginates into the distal segment, or the intussuscipiens (recipient segment) [7].
Intussusception can arise anywhere in the small intestine and colon. The terminology of intussusception reflects location of both the intussusceptum and intussuscipiens in the intestine: enteroenteric, appendiceal, appendiceal-ileocolic, ileocolic, colocolic, rectoanal, and stomal intussusception; rectoanal and stomal intussusception are considered as (extracorporeal) prolapse; and the coloanal intussusception can simulate a rectal prolapse and must be differentiated from rectal prolapse with careful clinical examination [8-10]. Whereas the majority of pediatric patients harbor a benign or physiologic process, 99% of adult intussusception patients harbor a pathological process [9].
Specifically, it is assessed that about 90% of intussusceptions in adults are secondary to an anatomic or pathologic disorder, of which more than half are malignant. Idiopathic cases, without a lead point lesion, are the exception in adults and make up 8-20% of cases [11]. Secondary intussusception is induced by organic lesions, including benign and malignant neoplasms, and metastatic cancers, inflammatory bowel disease, postoperative adhesions, Meckel’s diverticulum, or triggered iatrogenically due to the presence of intestinal tubes or jejunostomy feeding tubes after gastric surgery. Primary or idiopathic intussusception is frequently transient, whereas secondary intussusception due to a lead point is commonly permanent or recurrent [12]. About 20% of patients have no apparent etiology and are labelled as primary or idiopathic and intussusceptions without a lead point tend to be transient, self-limiting, and nonobstructing [8, 9].
To our knowledge, this is the first reported case of transient sigmoidorectal intussusception in an apparently healthy woman who underwent scheduled polypectomy. There are only a few reports describing transient intussusception. Regarding the small intestine, patients with Crohn’s and celiac diseases are known to present with transient adult intussusception commonly manifested as a non-lead point intussusception [13, 14]. Moreover, in a case of adult transient jejunojejunal intussusception without any underlying pathological lead point, surgical intervention yielded a negative laparotomy and resection was not required [15]. Regarding the colon, in a single cancer center, from 34 intussusceptions, seven were transient (i.e., intermittent) induced by edema due to portal hypertension in a patient with cholangioma, lipomas (2 patients), tubovillous adenoma (1 patient), colon cancer (1 patient), assumed sarcoma (1 patient) and presumed carcinoid (1 patient) [16].
Transient intussusception has also been reported as an incidental finding without any defined underlying cause for intussusception in patients with different basic disorders, such as aortic aneurysm, hepatic cyst or cerebral metastases [17].
In line with our rare case, the prevalence of intussusception is extremely low in the descending colon, owing to the descending colon anatomical attachment to the retroperitoneum. In adults, the exact mechanism of invagination of proximal colon into the distal colon is unidentified. It is supposed that any lesion in the bowel wall or within the lumen that modifies normal peristaltic activity is capable to initiate the process of intussusception. This theory, however, does not clarify the idiopathic cases of intussusception without any organic trigger [12].
Likewise, the exact mechanism of sigmoidorectal intussusception in our case is unidentified because there was neither a lesion in the colon nor an irritant in its lumen to serve as lead point that could change the normal peristalsis pattern and initiate the invagination leading to intussusception. In this respect, sigmoidorectal intussusception, a distinctly very rare condition in adult patients associated with a pathological cause, acts as the lead point in the mechanism of intussusception; benign or malignant lesions predominantly managed by surgical resection; and when the colon is involved, surgical resection is recommended owing to the high risk of underlying malignant tumor, perforation and spillage [6, 9].The peristalsis pushes the lesion, which functions as lead point, and leads to the intussusception of sigmoid in the rectal cavity.
The clinical presentation of adult colonic intussusception is mainly subacute or chronic, lasting several days or weeks, though acute presentations occasionally also occur. The symptomatology is often unspecific and may vary among individuals. Therefore, it is difficult to define an exact diagnostic algorithm. The most common presenting symptoms of sigmoidorectal intussusception include abdominal pain, nausea, vomiting and bleeding per rectum [3, 4, 18]. It must be emphasized that early diagnosis of sigmoidorectal intussusception is a diagnostic challenge because most cases present with non-specific signs and symptoms. In contrast, our own participant was free on any symptom from gastrointestinal tract.
Several imaging techniques could support the diagnosis of intussusception. There are employed examination methods, including plain abdominal X-rays, barium enema examination, colonoscopy, ultrasonography and CT. Abdominal CT appears to be the most useful tool for diagnosis of intussusception and is superior to other examination methods; it can reliably diagnose intussusception because of its virtually pathognomonic appearance, with the diagnostic accuracy of 83.3%; and it is able to distinguish between intussusception without a lead point (features: no signs of proximal bowel obstruction, target-like or sausage-shaped mass, layering effect) from that with a lead point (features: signs of bowel obstruction, bowel wall edema with loss of the classic 3-layer appearance, demonstration of a lead mass) [19]. This distinction is essential as it may help to decrease the number of unnecessary surgical interventions [20]. Likewise, CT remains the most reliable examination in making a preoperative diagnosis, to detect vascular compromise, and giving information about the possible extension of dissemination of a malignant tumor [21, 22]. With the increasing usage of imaging techniques and the overutilization of CT scans, idiopathic and asymptomatic intussusception could be diagnosed more often [15]. A water-soluble contrast enema shows a contrast-filled rectal cavity with a bowel loop floating and the characteristic finding of a cup-shaped [18].
Treatment of the large bowel intussusception commonly requires surgery since we have to consider about the possibility of an underlying pathologic process with possible malignant origin that could act as a lead point. The intussusception might be the initial and the only signal of the existence of a malignancy, very often colorectal carcinoma. Therefore, in case of the transient intussusception without any other subjective problems of a patient, presence of potential pathologic mass in the colon should be excluded.
Conclusion
To our knowledge a transient benign sigmoidorectal intussusception simulating submucosal tumor and its endoscopic picture has not been reported before in the literature.
Author Contributions
All authors participated in the case of the patient as well as in acquisition, analysis, or interpretation data. Moreover, all authors read, discussed the content and approved the final manuscript.
Conflicts of Interest
None.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Mon 06, Jan 2020Accepted: Tue 25, Feb 2020
Published: Sat 29, Feb 2020
Copyright
© 2023 Jannis Kountouras . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.02.13
Figures & Tables
References
- Mohamed M, Elghawy K, Scholten D, Wilson K, McCann M (2015) Adult sigmoidorectal intussusception related to colonic lipoma: A rare case report with an atypical presentation. Intern J Surg Case Rep 10: 134-137. [Crossref]
- Ongom PA, Opio CK, Kijjambu SC (2014) Presentation, aetiology and treatment of adult intussusception in a tertiary Sub-Saharan hospital: a 10-year retrospective study. BMC Gastroenterol 14: 86. [Crossref]
- Wang N, Cui XY, Liu Y, Long J, Xu YH et al. (2009) Adult intussusception: a retrospective review of 41 cases. W J Gastroenterol 15: 3303-3308. [Crossref]
- Zubaidi A, Al Saif F, Silverman R (2006) Adult intussusception: a retrospective review. Dis Colon Rectum 49: 1546-1551.
- Begos DG, Sandor A, Modlin IM (1997) The diagnosis and management of adult intussusception. Am J Surg 173: 88-94.
- Gueye ML, Sarr ISS, Gueye MN, Thiam O, Seck M et al. (2018) Adult ileocecal intussusception induced by adenomatous ileal polyp: case report and literature review. J Surg Case Rep 9: rjy256.
- Hassan WAW, Teoh W (2018) Intussusception after Colonoscopy: A Case Report and Review of Literature. Clin Endosc 51: 591-595.
- Valentini V, Buquicchio GL, Galluzzo M, Ianniello S, Di Grezia G et al. (2016) Intussusception in Adults: The Role of MDCT in the Identification of the Site and Cause of Obstruction. Gastroenterol Res Pract 2016: 5623718. [Crossref]
- Shenoy S (2017) Adult intussusception: A case series and review. World J Gastrointest Endosc 9: 220-227. [Crossref]
- Marinis A, Yiallourou A, Samanides L, Dafnios N, Anastasopoulos G et al. (2009) Intussusception of the bowel in adults: a review. World J Gagastroenterol 15: 407-411. [Crossref]
- Sclarovsky Benjaminov F, Wilson S, Habal F (2003) Adult celiac disease presenting with intussusception and elevated liver enzymes. Isr Med Assoc J 5: 203-204.
- Khan Z, Darr U, Renno A, Alkully T, Rafiq E et al. (2017) Transient Descending Colocolonic Intussusception Due to a Large Fecaloma in an Adult. ACG Case Rep J 4: e94. [Crossref]
- Knowles MC, Fishman EK, Kuhlman JE, Bayless TM (1989) Transient intussusception in Crohn disease: CT evaluation. Radiology 170: 814. [Crossref]
- Willingham FF, Opekun AR, Graham DY (2003) Endoscopic demonstration of transient small bowel intussusception in a patient with adult celiac disease. Gastroint Endosc 57: 626-627.
- Lai J, Ramai D, Murphy T, Kasher F (2017) Transient Adult Jejunojejunal Intussusception: A Case of Conservative Management vs. Surgery. Gastroenterol Res 10: 369-371. [Crossref]
- Gollub MJ (2011) Colonic intussusception: clinical and radiographic features. Am J Roentgenol 196: W580-W585.
- Catalano O (1997) Transient small bowel intussusception: CT findings in adults. Brit J Radiol 70: 805-808.
- Choi SH, Han JK, Kim SH, Lee JM, Lee KH et al. (2004) Intussusception in adults: from stomach to rectum. Am J Roentgenol 183: 691-698. [Crossref]
- Yakan S, Caliskan C, Makay O, Denecli AG, Korkut MA (2009) Intussusception in adults: clinical characteristics, diagnosis and operative strategies. World J Gastroenterol 15: 1985-1989. [Crossref]
- Kim YH, Blake MA, Harisinghani MG, Archer Arroyo K, Hahn PF et al. (2006) Adult intestinal intussusception: CT appearances and identification of a causative lead point. Radiographics 26: 733-744.
- Beattie GC, Peters RT, Guy S, Mendelson RM (2007) Computed tomography in the assessment of suspected large bowel obstruction. ANZ J Surg 77: 160-165.
- Gayer G, Zissin R, Apter S, Papa M, Hertz M (2002) Pictorial review: adult intussusception - a CT diagnosis. Brit J Radiol 75: 185-190.