Surgical Management of a Breast Liposarcoma Arising in An Elderly Male with An Overlying Permanent Pacemaker: A Case Report with Associated Radiologic and Intraoperative Imaging
A B S T R A C T
Liposarcomas are rare tumors. Here we present a case of a 90-year-old male who was found to have a rapidly enlarging left breast mass. PET CT imaging demonstrated a large mass arising between the pectoralis major and minor. Ultrasound guided core biopsy results reported spindle cells. Wide excision was performed with use of harmonic energy device due to the patient’s overlying pacemaker. Histologic analysis confirmed high grade dedifferentiated liposarcoma.
Keywords
Soft tissue sarcoma , liposarcoma, surgical resection
Introduction
Soft tissue sarcomas are rare malignant tumors originating from mesenchymal tissue that can appear in any anatomic location. There is a higher proportion found in the extremities, but they can also be found arising from breast adipose and connective tissue components [1]. Breast sarcomas are extremely rare especially when found in men as these account for 1.5 percent of breast sarcoma cases [2]. Obtaining a tissue diagnosis along with histologic grading are crucial for prognosis and management of breast sarcomas [3]. Here we discuss a rare case of dedifferentiated liposarcoma arising between the pectoralis major and minor muscles in an elderly male with an overlying permanent pacemaker. Clinical features, diagnostic evaluation, and surgical management of the patient are discussed. Associated radiologic and intraoperative images are included along with a brief discussion of the relevant literature.
Case
A 90-year male with history of tachycardia-bradycardia syndrome status post left pacemaker placement who presented with a rapidly enlarging, painful mass of his left chest over a three-month period. On physical exam the mass was noted to be solid and mobile with no skin retraction, nipple discharge or bleeding. No palpable axillary lymph nodes were present on exam (Figure 1). The mass was slightly tender to palpation. Initial work up consisted of a non-contrast enhanced chest CT which demonstrated a left anterior chest mass measuring 9.6 x 6.5 x 6.8 cm arising between the left pectoralis major and minor muscles (Figure 2). Duplex ultrasound with doppler flow of the left breast mass revealed a 9.7 x 6.5 x 6.1 cm hypoechoic lesion with internal vascularity. Ultrasound guided core biopsies revealed atypical spindle cell tumor. Due to the rapid enlargement of this mass and the initial pathology showing atypical spindle cell tumor, a PET CT scan was ordered to stage this soft tissue sarcoma. The PET CT (Figure 3) showed an 8 x 8 cm mass posterior to the lateral aspect of the left pectoralis major muscle with maximum SUV of 15.3. The central area of the mass was cold suggesting necrosis. No other abnormal uptake was seen.
The pacemaker pocket was felt to be distinctly separate from the underlying mass both clinically and radiologically and thus a preoperative electrophysiology consult was not obtained. The plan was to use the harmonic scalpel to obviate any hemodynamic effects of pacemaker inhibition. A post-operative cardiology consult was obtained for interrogation of the pacemaker. The patient underwent a wide excision and en bloc resection of the mass along with pectoralis major and minor (Figure 4, 5, 6, 7). Intraoperatively the axillary vein, long thoracic nerve, and thoraco-dorsal artery and nerve were identified and protected. A hemovac drain was placed and closure was achieved with 2-0 vicryl and skin staples.
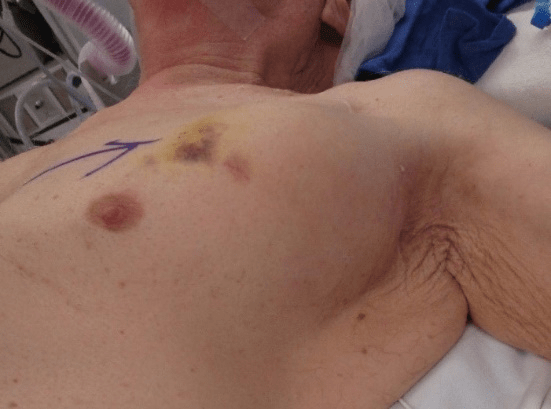
Figure 1: Preoperative view of large breast mass.
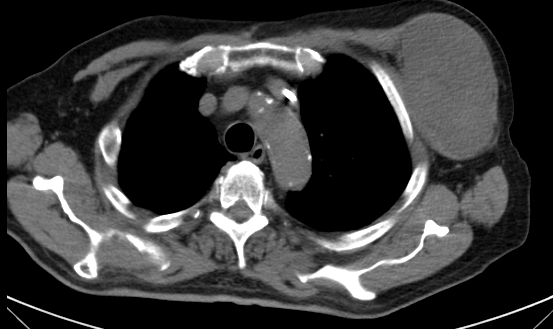
Figure 2: CT imaging demonstrates a large anterior chest mass arising between the pec major and minor muscles.
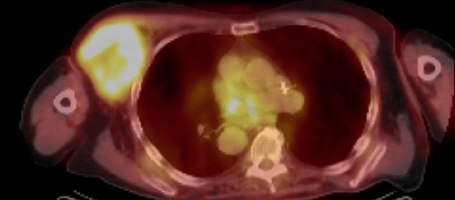
Figure 3: 8 x 8 cm mass posterior to the left pectoralis major muscle with maximum SUV of 15.3. The central area of the mass was cold suggesting necrosis.
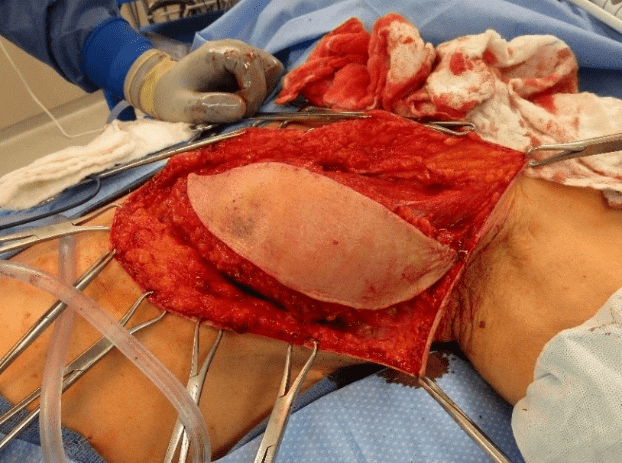
Figure 4
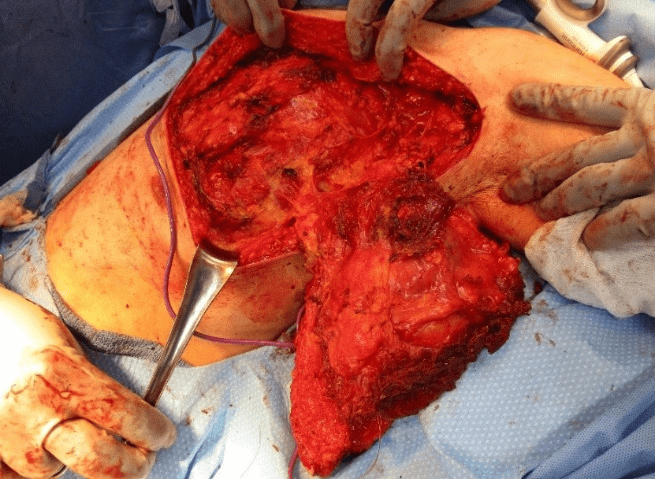
Figure 5
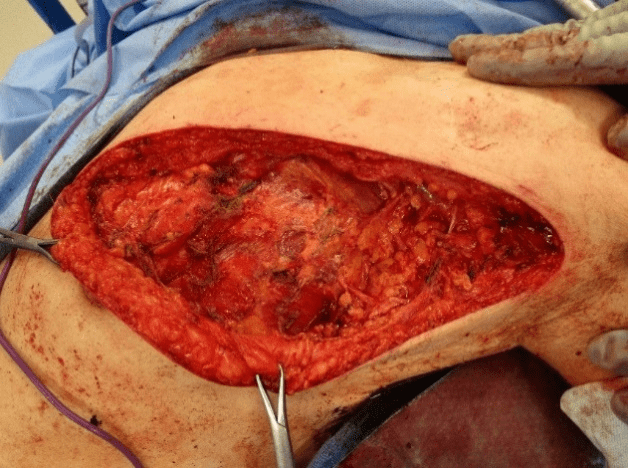
Figure 6
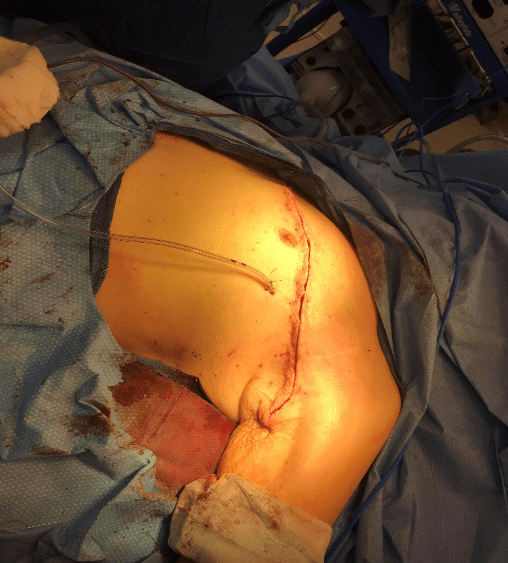
Figure 7
Gross pathologic specimens can be seen in (Figure 8). The final histopathologic diagnosis was High grade dedifferentiated liposarcoma with necrosis present and a mitotic rate >19/10 high-power fields. The inferior margins were found to be involved microscopically (R1). The postoperative course was uneventful and the Hemovac drain was pulled at the first post-op visit. The post-operative treatment plan involved locoregional radiation therapy for which the patient required implantation of a right-sided permanent pacemaker due to the left pacemaker being in the field of radiation.
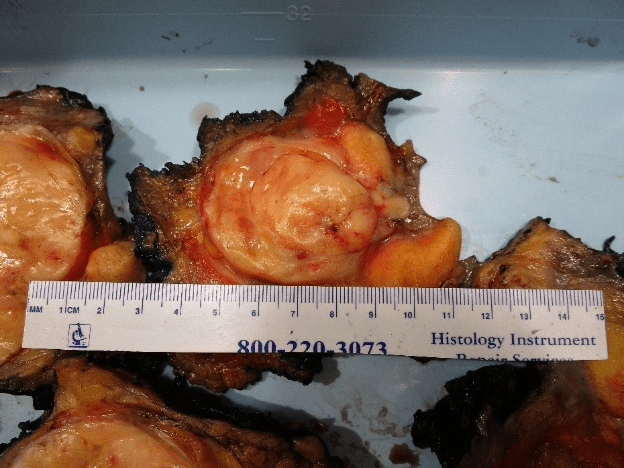
Figure 8
Discussion
Liposarcoma is the most common soft-tissue sarcoma encountered, with dedifferentiated liposarcoma usually arising in the retroperitoneum [4, 5]. 10 % of well-differentiated liposarcomas can have a component of dedifferentiation. Molecular studies can characterize and assist in diagnosis of dedifferentiated liposarcoma. MDM2 and CDK4 is positive in dedifferentiated liposarcoma and negative in myxoid and pleomorphic liposarcomas. Supernumerary rings and/or giant rod chromosomes that contain amplified sequences of the region 12q14-15 are characteristic of dedifferentiated liposarcoma [5].
Rapidly enlarging breast masses in male patients should raise the suspicion for a soft tissue malignancy and targeted imaging and biopsies should be obtained. Incisional, excisional, or core biopsies can all provide adequate tissue samples but core biopsy with image guidance is considered the procedure of choice in most instances. Mammography can be non-specific for primary breast sarcomas as calcifications and spiculations are usually absent. CT, MRI and PET/CT are all recommended for further evaluation of underlying vascularity and metastases and help in surgical planning. [6].
Here we encountered a rare case in which an elderly male with no history of prior trauma presented with a large painful left breast dedifferentiated liposarcoma deep to a permanent pacemaker pocket. Principles of management in these rare instances includes imaging studies to assess vascularity of the underlying mass and abutment/invasion of pacemaker pocket. Care should be taken when using electrocautery with use of low energy, short electrocautery bursts to minimize any hemodynamic effects of pacemaker inhibition or to use new energy devices such as the harmonic scalpel energy system. Post-op interrogation of cardiac devices is recommended [7].
Article Info
Article Type
Case ReportPublication history
Received: Thu 27, Jun 2019Accepted: Wed 16, Oct 2019
Published: Wed 30, Oct 2019
Copyright
© 2023 Francisco Benavides. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2019.04.14
Figures & Tables
References
- Duncan Mallory, L M (2018) Sarcomas of the Breast. Surgical Clinics of North America 869-876.
- Adem C, Reynolds C, Ingle JN, Nascimento AG (2004) Primary breast sarcoma: clinicopathologic series from the Mayo Clinic and review of the literature. Br J Cancer 91: 237-241. [Crossref]
- Dei Tos AP, P F (2002) Atypical lipomatous tumor/well differentiated liposarcoma. World Health Organization Classification of Tumors: Pathology and Genetics of Tumors of Soft Tissue and Bone 35-37.
- Italiano A, Toulmonde M, Cioffi A, Penel N, Isambert N et al. (2012) Advanced well-differentiated/ dedifferentiated liposarcomas: role of chemotherapy and survival. Ann Oncol 23: 1601-1607. [Crossref]
- Livingston JA, Bugano D, Barbo A, Lin H, Madewell JE et al. (2017) Role of chemotherapy in dedifferentiated liposarcoma of the retroperitoneum: defining the benefit and challenges of the standard. Sci Rep 7: 11836. [Crossref]
- Salemis NS (2015) Intramuscular Atypical Lipomatous Tumor/Well-Differentiated Liposarcoma of the Pectoralis Major Masquerading as a Breast Tumor: Management and Review of the Literature. Int Surg 100: 194-198. [Crossref]
- Levine PA, Balady GJ, Lazar HL, Belott PH, Roberts AJ (1986) Electrocautery and pacemakers: management of the paced patient subject to electrocautery. Ann Thorac Surg 41: 313-317. [Crossref]