Journals
Superior Vena Cava Obstruction Secondary to Prolonged Calcium Therapy: A Benign Etiology, Managed by Vein Graft Bypass Surgery
A B S T R A C T
We like to report this case of a 28-year-old lady, who had celiac disease and developed complete Superior Vena Cava Obstruction secondary to prolonged corrective calcium therapy for refractory Hypocalcemia through the central venous line. Usually Superior Vena Cava Syndrome (SVCS) due to Superior Vena Cava obstruction (SVCO) has infective and malignant etiologies. Our case is a rare and benign cause, managed surgically after failed endovascular recanalization by the interventional radiologist.
Keywords
SVC syndrome, calcium therapy, celiac disease, saphenous vein graft
Introduction
The superior vena cava is a large valve less vein, with a diameter up to 2 cm and a length of approximately 7 cm. The superior vena cava is formed by the union of left and right brachiocephalic veins and drains into the right atrium. This allows the right heart pressure to be conducted upwards into the right internal jugular vein, a common site of central venous access [1]. The first case of SVCS was reported in the medical literature by William Hunter in 1757 [2]. A couple of decades earlier the common causes were, infectious diseases like tuberculosis, syphilis, fibrosing mediastinitis and aortic aneurysms. With the advent of modern antimicrobial regimens, now the leading causes of SVCS are malignant disorders (Table 1) [3]. The increasing use of central venous access for lines and pacemakers, is contributing to the rare causes of SVCO. Prolonged calcium therapy administered via central is reported less in the literature.
Table 1: Common etiologies of superior vena cava syndrome.
|
Malignant (>85%) |
BENIGN (3% to 15%) |
|
Lung cancer |
Indwelling catheters |
|
Lymphoma |
Thymoma |
|
Breast Cancer |
Cystic Hygroma |
|
|
Tuberculosis |
|
|
Histoplasmosis |
|
|
Thyroid goiter |
|
|
Aortic aneurysm |
Case Report
A 28-year-old lady a known case of celiac disease with persistent hypocalcemia refractory to oral calcium replacement therapy. So, she frequently received calcium gluconate through the right jugular venous catheter for about 4 weeks. Afterwards she developed facial swelling, plethora, headaches, dry cough and orthopnea. There was dizziness and head spinning sensation on bending the head forwards. Examination showed distended neck and upper trunk veins. CT angiogram revealed complete obstruction of SVC and formation of upper trunk venous collaterals. (Figure 1).
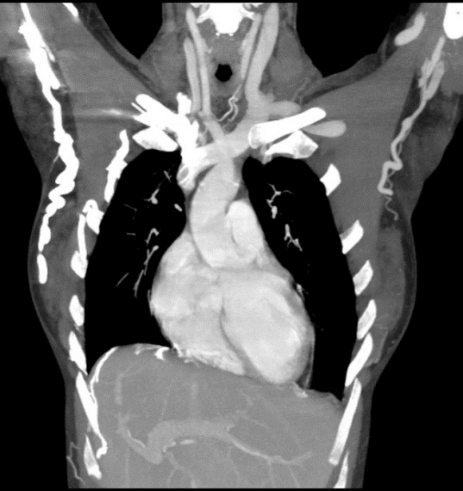
Figure 1: CT scan Thorax (Coronal view) showing complete obstruction of SVC.
Endovascular recanalization (dilatation and stenting) unsuccessful, as the interventional radiologist were unable to pass the guide wire through the occluded superior vena cava (SVC). The patient was finally referred to us for surgical management. Full sternotomy revealed fibrosed and thickened superior vena cava. Left great sephanous vein was harvested and opened in the longitudinal fashion, all valves were removed, and a graft was constructed over a 32 Fr chest drain using 7-0 prolene non absorbable sutures (Figure 2).

Figure 2: Saphenous vein spiral graft construction.
This modulated vein graft was anastomosed proximally to the left brachiocephalic vein and distally to the right atrial appendage. Upon releasing the vascular clamps, the graft filled up nicely (Figure 3). Intraoperative Doppler studies confirmed excellent run off in the graft. Sternotomy closed with five number 5 steel wires. She was extubated on table and the postoperative course was eventless. There was dramatic clinical improvement and was sent home on oral anticoagulants (Warfarin).
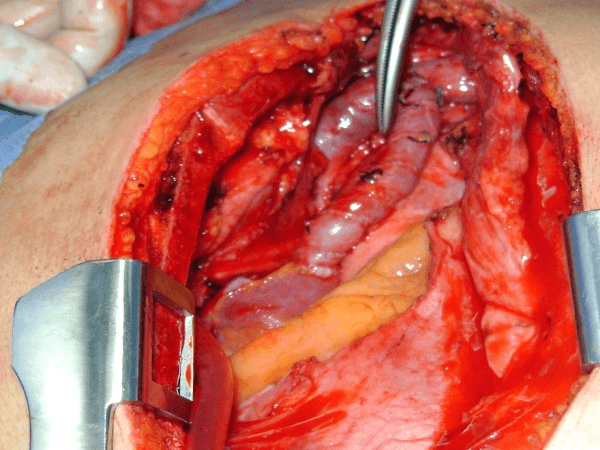
Figure 3: Spiral saphenous vein graft anastomosis from Innominate vein to right atrial appendage.
Discussion
To determine the treatment modalities, underlying cause of the superior vena cava syndrome must be considered. The Oncological diseases like, Bronchogenic carcinoma. Non-Hodgkin’s Lymphoma, Thyroid carcinoma and metastatic mediastinal tumors are managed with radiation therapy as well as systemic chemotherapy and usually respond well [4-6]. Endovascular recanalization (stenting & dilations) by the interventional radiologist as the main stay of management for short segments of occlusion [7, 8]. Surgical bypass is reserved for patients with benign etiology and in very limited oncological cases. Preoperative diagnosis of complete SVC obstruction with CT Venography is mandatory.
Dotty et al. have classified SVCO into 4 types, Stanford Dotty Classification:
i. Type 1 < 90% SVC stenosis and patent azygos vein.
ii. Type II 90-100 % stenosis and patent azygos vein.
iii. Type III 90-100 % stenosis of SVC with reverse circulation in patent azygos vein.
iv. Type IV Total occlusion of SVC and its supplying veins [9].
It is recommended to do the surgical bypass in Type III and type IV along with selected severely symptomatic case of Type II as well. Sometime surgical procedure is indicated after technical failure regarding radiological intervention. There is another known clinical classification of SVC syndrome intensity grading system (Table 2).
Table 2: Classification of SVC syndrome using the YALE SVC syndrome grading system [10].
|
Severity Class |
YALE Definition |
|
0 |
Asymptomatic: radiographic SVC obstruction in the absence of symptoms |
|
1 |
Mild: edema in the head or neck, cyanosis, plethora |
|
2 |
Moderate: edema in the head or neck with functional impairment |
|
3 |
Severe: mild to moderate cerebral edema, laryngeal edema, or diminished cardiac reserve |
|
4 |
Life-threatening: significant cerebral edema, laryngeal edema, or hemodynamic compromise |
|
5 |
Fatal: causing death |
Conclusion
Tailoring the treatment and management of SVCO according to the etiology is of prime importance. The Oncological cases are mainly treated with chemotherapy, radiotherapy or both modalities. If a small segment is involved then endovascular interventions, i.e., stent implantation, dilatation might be successful in 90-100 % of the cases. However, in some cases SVC thrombolysis and later dilatation and stent placement is associated with a risk of substantial hemorrhage in 10-15 % of the procedures. If we run out of all available less invasive treatment options and conservation, especially in benign causes [11]. Surgical bypass remains the resort of choice. Bypassing the occlusion using autologous sephanous vein graft is a good option and long-term good results have been reported in the literature [12].
In our case calcium replacement therapy over an extended period via central venous catheter led to complete SVC occlusion likely due to the sclerosing effect of calcium [13].
Conflicts of Interest
None.
Funding
None.
Consent
Consent was taken from patient.
Article Info
Article Type
Case ReportPublication history
Received: Mon 29, Jun 2020Accepted: Thu 16, Jul 2020
Published: Sat 01, Aug 2020
Copyright
© 2023 Ahsan Iqbal Cheema. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.08.01
Author Info
Corresponding Author
Ahsan Iqbal CheemaDepartment of Thoracic Surgery, King Fahad Specialist Hospital, Dammam, Saudi Arabia
Figures & Tables
Table 1: Common etiologies of superior vena cava syndrome.
|
Malignant (>85%) |
BENIGN (3% to 15%) |
|
Lung cancer |
Indwelling catheters |
|
Lymphoma |
Thymoma |
|
Breast Cancer |
Cystic Hygroma |
|
|
Tuberculosis |
|
|
Histoplasmosis |
|
|
Thyroid goiter |
|
|
Aortic aneurysm |
Table 2: Classification of SVC syndrome using the YALE SVC syndrome grading system [10].
|
Severity Class |
YALE Definition |
|
0 |
Asymptomatic: radiographic SVC obstruction in the absence of symptoms |
|
1 |
Mild: edema in the head or neck, cyanosis, plethora |
|
2 |
Moderate: edema in the head or neck with functional impairment |
|
3 |
Severe: mild to moderate cerebral edema, laryngeal edema, or diminished cardiac reserve |
|
4 |
Life-threatening: significant cerebral edema, laryngeal edema, or hemodynamic compromise |
|
5 |
Fatal: causing death |
References
- Hunter J White, Michael P Soos (2019) Anatomy, Thorax, Superior Vena Cava. StatPearls. [Crossref]
- Doty DB, Jones KW (1996) Superior vena cava syndrome. In Glen’s Thoracic and cardiovascular surgery 6th ed. Baue AE, Geha AS, Hammond GL et al, eds Stamford. CT: Appleton and Lange 595-602.
- Ronny Cohen, Derrick Mena, Roger Carbajal Mendoza, Ninon Matos, Nishu Karki (2008) Superior vena cava syndrome: A medical emergency? Int J Angiol 17: 43-46. [Crossref]
- C P Escalante (1993) Causes and management of superior vena cava syndrome. Oncology 7: 61-68. [Crossref]
- B A Armstrong, C A Perez, J R Simpson, M A Hederman (1987) Role of irradiation in the management of superior vena cava syndrome. Int J Radiat Oncol Biol Phys 13: 531-539. [Crossref]
- N P Rowell, F V Gleeson (2002) Steroids, radiotherapy, chemotherapy and stents for superior vena caval obstruction in carcinoma of bronchus a systemic review. Clin Oncol 14: 338-351. [Crossref]
- Adnan Z Rizvi, Manju Kalra, Haraldur Bjarnason, Thomas C Bower, Cathy Schleck et al. (2008) Benign superior vena cava syndrome: stenting is now the first line of treatment. J Vasc Surg 47: 372-380. [Crossref]
- Manju Kalra, Indrani Sen, Peter Gloviczki (2018) Endovenous and Operative Treatment of Superior Vena Cava Syndrome. Surg Clin North Am 98: 321-335. [Crossref]
- J R Doty, J H Flores, D B Doty (1999) Superior vena cava obstruction using spiral vein graft. Ann Thorac Surg 67: 1111-1116. [Crossref]
- Emma B Holliday, David A Hampton, Charles R Thomas Jr, Shushan Rana (2016) Prognostic value of the Yale Grading system for Superior Vena Cava Syndrome. Ann Am Thorac Soc 13: 1862-1865. [Crossref]
- Michele Gallo, Adam N Protos, Jaimin R Trivedi, Mark S Slaughter (2016) Surgical treatment of benign superior vena cava syndrome. Ann Thorac Surg 102: e369-e371. [Crossref]
- D B Doty, J R Doty, K W Jones Jones (1990) K.W: By-pass of superior vena cava. Fifteen years’ experience with spiral vein graft for obstruction of superior vena cava caused by benign disease. J Thorac Cardiovasc Surg 99: 889-895. [Crossref]
- Elio Venturini, Lucia Becuzzi, Lucia Magni (2012) Catheter- induced Thrombosis of the Superior vena Cava. Case Rep Vasc Med 2012: 469619. [Crossref]