Journals
Spontaneous Cervical Cerebrospinal Fluid Leakage Leading to Intracranial Hypotension
A B S T R A C T
This is a case of intracranial hypotension presented with postural headache and imaging study showed typical findings of leptomeningeal enhancement, subdural effusion, and brain sag. Further workup showed cervical cerebrospinal fluid leakage. Surgical treatment was successfully performed to repair the leakage after blood patch failure.
Keywords
Spontaneous intracranial hypotension, subdural effusion, cerebrospinal fluid leakage, surgical repair.
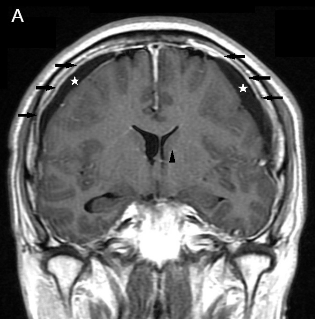
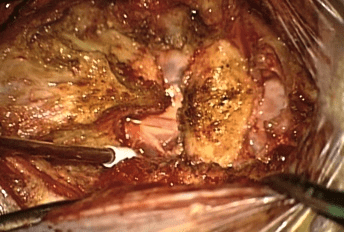
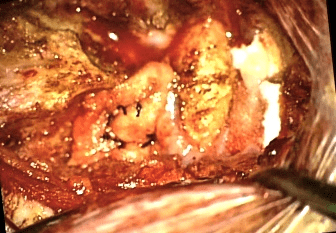
A 47-year-old man with tonsillar cancer, status post tonsillectomy and concurrent chemoradiotherapy presented with a seven-day history of progressive headache that was exacerbated by the upright position and relived by lying down. The symptom was not relived by pain killer and the consciousness became drowsy. Magnetic resonance imaging (MRI) revealed diffuse meningeal enhancement, and subdural effusion (Figure 1A). Spontaneous intracranial hypotension was impressed and cerebrospinal fluid leakage over C1-C2 interlaminar space with cerebellar tonsilar hernation suggestive of the “brain sag” was found on MRI myelography (Figure 1B). After failure of conservative measures, he underwent burr hole drainage of bilateral subdural effusion and surgical repair of the dural defect on C1-C2 interlaminar space (Figure 2A) with paraspinal fascia (Figure 2B). He regained consciousness after surgical treatment, and the symptom of orthostatic headache gradually resolved.
Spontaneous intracranial hypotension is often misdiagnosed; physicians should be aware of this possibility in patients with orthostatic headache and typical imaging findings [1]. These spontaneous cerebrospinal fluid leakages may be due to minor trauma or pre-existing dural weakness [1]. CSF leaks are most frequently located at the thoracic level of the spine while leakage sites over C1-C2 level were also documented in many case reports [2, 3]. Epidural blood patching, percutaneous injection of fibrin glue, and surgical repair are the choice of treatment. Without the correct diagnosis, one may drain the effusion only without repairing the dural defect to prevent further leakage. This may lead to recurrence of the subdural effusion.

Article Info
Article History
Research ArticlePublication history
Received: 16 April, 2019Accepted: 27 April, 2019
Published: 10 May, 2019
Copyright
© 2018 S. Dar-Ming Lai. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository. All rights reserved.DOI: 10.31487/j.SSG.2018.01.04
Author Info
Corresponding author
Dar-Ming LaiM.D. Ph D, Division of Neurosurgery, Department of Surgery, National Taiwan University Hospital and National Taiwan University College of Medicine, 7 Chung Shan South Road, Taipei 100, Taiwan.
Figures & Tables
References
- Inamasu J, Guiot BH (2006) Intracranial hypotension with spinal pathology. Spine J 6: 591-599. [Crossref]
- Rai A, Rosen C, Carpenter J, Miele V (2005) Epidural blood patch at C2: diagnosis and treatment of spontaneous intracranial hypotension. AJNR Am J Neuroradiol 26: 2663-2666. [Crossref]
- Peng PW, Farb R (2008) Spontaneous C1–2 CSF leak treated with high cervical epidural blood patch. Can J Neurol Sci 35: 102-105. [Crossref]