Spinal Myxoma of the Facet Joint: A Case Report
A B S T R A C T
Myxoma is a benign soft tissue tumor that can occur in a variety of locations. Intramuscular localization is common, myxomas of the paravertebral muscle are relatively rare and only few cases have been described in literature. Juxta-articular myxoma on facet joint is extraordinary. The current case described paraspinal muscles juxta-articular myxoma of the lumbar region in a 61-year-old man causing back pain and sciatica. Radiological findings showed a mass in the nearby of L5-S1 facet joints mimicking a big synovial cyst that deepened down into the psoas major muscle. A PET scan showed a higher metabolism involving the mass and no other localizations. Intraoperative histological analysis was consistent with Juxta-articular myxoma (JM). Treatment of choice was surgical excision, with complete relief of symptoms afterwards.
Keywords
Myxoma, intramuscular myxoma, juxta-articular myxoma, spine surgery
Introduction
Myxoma is a benign, slow-growing soft tissue tumor of mesenchymal origin. The estimated incidence is at one case/million population/year [1]. Even if commonly found in the left atrium of the heart, myxomas can arise in many different districts, such as large muscles (Intramuscular Myxoma) and even in continuity with joints (Juxta-articular Myxoma). Myxomas appear as ovoid painless masses often containing cystic areas. Size can range from 1-17 cm but more commonly they have been found smaller than 5cm in length, thus larger size often needs further investigations, and an alternative diagnosis should be taken into account [2-4]. Symptoms can occur consequently to the compression on adjacent structures (vascular, neurological). Neurological symptoms such as cord compressions or nerve root compression, are rare [5]. Only 5 cases of juxta-articular myxomas of paraspinal are described in literature. We report a case of a juxta-articular myxoma in the lumbar spine causing back lumbar pain. MRI of the lumbar spine showed a big multilobulated mass at L5-S1 within paraspinal muscles, hypointense in T1-weithed sequences and hyperintense in T2-weighted. The neoplasia could have been mistaken for a giant synovial cyst due to the involvement of facet joints. Since the uncommon presentation and uncharacteristically large size, a PET-scan was conducted in order to rule out the eventuality of systematic disease. Intraoperative histological examination yielded the diagnosis towards a benign neoformation so surgical excision was conducted.
Case Presentation
I Patient Description and Case History
A 61-year-old man, height 180 cm, weight 75 kg, without relevant comorbidities and pharmacotherapies, had experienced low-back pain over 1 year, which worsened in last 4-month with irradiation down the right leg (L5 root).
II Physical Examination Results
Physical examination revealed a palpable mass on the right paraspinal area in the lumbar region. Neurological examination demonstrated normal strength (5/5) in all muscle groups in both legs. Wasserman and Lasegue tested positive on the right side. The patient presented with no further deficits.
III Results of Pathological Tests and Other Investigations
In January 2020, a pelvis CT study of the lumbosacral region revealed multiple hypodense paravertebral formations, referable to joint cysts (Figures 1 & 2). F18G-PET showed a hypermetabolic area (SUV max 3.0) on the right paravertebral muscles at L5-S1 level deepening into the right psoas major muscle.
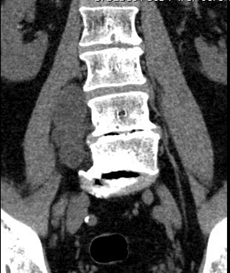
Figure 1: Coronal CT scan of lumbosacral spine.
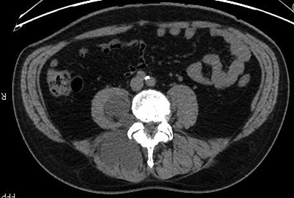
Figure 2: Axial CT scan.
A pelvis MRI confirmed a multilobulated mass involving the right paravertebral muscles in the lower lumbar and sacral region that appeared hypodense on T1-weighted sequences and hyperdense in T2-weighted sequences (Figures 3 & 4).
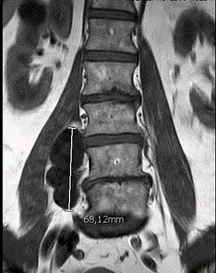
Figure 3: Coronal MR image of lumbosacral spine show hypointense paravertebral lesion (T1 signal).

Figure 4: Axial MR image of lumbosacral spine show contrast-enhanced of the lesion (T2 signal).
IV Treatment Plan
In October 2020, a core needle biopsy of the right paravertebral muscle was conducted with non-diagnostic result. In January 2021 he underwent surgical treatment to perform an extemporaneous incisional biopsy and eventual excision of the tumor. A posterior access was performed. The tumor appeared as an encapsulated gray-white mass inside paraspinal muscles (Figure 5). The freezer histological exam confirmed a benign tumor so the dorsal portion was removed through a good cleavage plan. A clear mucinous fluid flowed from the remaining ventral part of the tumor was removed.
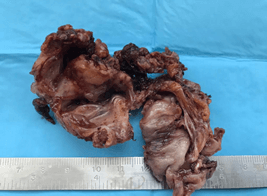
Figure 5: Specimen after resection.
V Pathological Examination
The histological examination was consistent for an intramuscular myxoma with cystic areas degeneration. (CD34 - / +, EMA-, MUC4, S100-, SOX10-).
VI Expected Outcome of the Treatment Plan
The patient recovered easily from the procedure. Immediately postoperatively, he experienced complete relief from symptoms.
Discussion
Myxoma is a benign mesenchymal tumor. The term myxoma is used to identify a plethora of tumor which can occur in every part of the body. The term was first used to describe lesions that mimic the structure of umbilical cord. Myxomas are composed by a paucity of stellate cells set in a loose myxoid stroma with, minimal mitotic figures [3]. It is a rare condition and its incidence is reported to be one per million individuals, most frequently diagnosed in female patients between 40-70 years [6]. Allen extensively described multiple variants of this tumor and he identified several subgroups of the so called “mainstream soft-tissue myxomas”; Among them Intramuscular Myxoma (IMM) is the most common form of myxoma after myocardial myxoma and can be located in any skeletal muscle groups. IMM is a solitary tumor, but it could present as part of Mazbraud’s syndrome, in which multiple myxomas associate with fibrous dysplasia in one or more bones [7]. IMM is typically seen as a well-circumscribed intramuscular mass. Magnetic resonance shows low-signal intensity in T1-weighted scan, hypointense to muscle; T2-weighted MRI displays as homogeneous, hyperintense to muscle and brighter than fat; STIR (short T1 inversion recovery) shows high-signal intensity with a surrounding fat rim [8].
On PET/CT myxoma could show 18-FDG avidity [9]. A specific variant of myxoma, resembling an IMM in almost every radiological and histological aspects, is the Juxta-articular myxoma (JAM): this tumor origin in the nearby and involves periarticular tendons, ligaments and joint capsules. JAM can indeed be histologically indistinguishable from the intramuscular form, and especially when the juxta-articular myxoma invades muscle, it may be impossible to differentiate the two on the basis of the section. Macroscopically myxomas arising from joints tend to present more focal vascularity, peripheral fibroblastic proliferation and more cystic areas than IMM. Cysts of varying sizes resembling ganglion cysts are seen in 89% of cases[10]. Given the close relationship to joints and its ganglion-like cystic spaces, this condition is closely related to ganglion cysts, which are a rather rare event. IMM, as aforementioned is completely benign and no recurrences have been described in the literature. Conservative treatment is the gold standard while excision is to be considered when symptomatic. On the other hand, JAM presents a higher risk of recurrences. Meis and Enziger reported 34% of recurrence in their study. In the case presented, the patient suffered from radicular pain due to the mechanic effect of the mass against the nerve root. Thus, we decided to remove the tumor.
In order to remove the whole mass, including the ventral portion within the psoas major muscle, a combined surgical approach should have been conducted, with higher rate of intraoperative complications. Given the benign nature of intraoperative histological exams we opted to remove only the portion causing the compression and symptoms, avoiding a longer and unnecessary procedure.
Conflicts of Interest
I hereby certify, to the best of my knowledge that the authors listed in the case report presented have no affiliations with or involvement in any organization or entity with any financial interest, or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Article Info
Article Type
Case ReportPublication history
Received: Tue 26, Jan 2021Accepted: Sat 13, Feb 2021
Published: Sat 27, Feb 2021
Copyright
© 2023 S. Colangeli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.02.19
Figures & Tables
References
1. Miettinen M, Hockerstedt K, Reitamo J, Totterman S (1985) Intramuscular myxoma -- a clinicopathological study of twenty-three cases. Am J Clin Pathol 84: 265-272. [Crossref]
2. Petscavage Thomas JM, Walker EA, Logie CI, Clarke LE, Duryea DM et al. (2014) Soft-tissue myxomatous lesions: Review of salient imaging features with pathologic comparison. Radiographics 34: 964-980. [Crossref]
3. Allen PW (2000) Myxoma is not a single entity: a review of the concept of myxoma. Ann Diagn Pathol 4: 99-123. [Crossref]
4. Shugar JMA, Som PM, Meyers RJ, Schaeffer BT (1987) Intramuscular Head and Neck Myxoma. Laryngoscope 97: 105-107. [Crossref]
5. Guppy KH, Wagner F, Tawk R, Gallagher L (2001) Intramuscular myxoma causing lumbar radiculopathy. J Neurosurg 95: 260-263. [Crossref]
6. Charron P, Smith J (2004) Intramuscular myxomas: a clinicopathologic study with emphasis on surgical management. Am Surg 70: 1073-1077. [Crossref]
7. Kabukcuoglu F, Kabukcuoglu Y, Yilmaz B, Erdem Y, Evren I (2004) Mazabraud’s syndrome: Intramuscular myxoma associated with fibrous dysplasia. Pathol Oncol Res 10: 121-123. [Crossref]
8. Bancroft LW, Kransdorf MJ, Menke DM, O’Connor MI, Foster WC (2002) Intramuscular myxoma: Characteristic MR imaging features. AJR Am J Roentgenol 178: 1255-1259. [Crossref]
9. Nishio J, Naito M (2012) FDG PET/CT and MR imaging of intramuscular myxoma in the gluteus maximus. World J Surg Oncol 10: 132. [Crossref]
10. Meis JM, Enzinger FM (1992) Juxta-articular myxoma: A clinical and pathologic study of 65 cases. Hum Pathol 23: 639-646. [Crossref]