Small Bowel Obstruction Due to a Gossypiboma: A Rare and Dreaded Sequel of a Trauma Laparotomy
Small Bowel Obstruction Due to a Gossypiboma: A Rare and Dreaded Sequel of a Trauma Laparotomy
A B S T R A C T
This is a case report of a 23-year-old male who presented to a hospital in Aleppo with a few months’ history of abdominal pain and diarrhea associated with progressive weight loss and ultimate cachexia. Patient’s history is significant for a trauma laparotomy due to a blast injury with management of a colonic and orthopedic injuries. Three months later he underwent a second laparotomy for reversal of the stoma after which his symptoms started and gradually became worse. The abdominal pain attacks were so severe unresponsive to analgesics and he had lost around 30 kg. He underwent CT scan on presentation which showed small bowel obstruction and was taken down to the operating room (OR) for exploration. In the operating room a hard mass was palpated in the small bowel and a small enterotomy was done overlying the mass with retrieval of a large surgical pad, gossypiboma, from the lumen. The enterotomy was closed primarily and the patient did well postoperatively and was discharged home.
Keywords
Gossypiboma, obstruction, trauma, laparotomy
Introduction
Small bowel obstruction (SBO) is a common cause of admission to the surgical wards and the incidence of small bowel obstruction due to adhesive bands is up to 3% after laparotomies [1]. The most common cause of SBO is due to adhesions in up to 74% of cases and the second most common cause are tumors, mainly metastatic, in up to 20% [2, 3]. The incidence of retained surgical pads also known as gossypiboma or textiloma is reported to be around 1 in 1000-1500 cases and they can have a spectrum of presentations [4]. They can present as intra-abdominal abscesses or intestinal fistulae or can remain asymptomatic for years and present later mimicking tumors or causing perforation or obstruction [5-7]. Here is a case of a gossypiboma with intraluminal migration into the small bowel causing obstruction in a young male after a trauma laparotomy in the war-laden zone of Syria.
Case Presentation
This is a case of a 23-year-old male, previously healthy who presented to a tertiary care hospital in Aleppo on March of 2016 with a few months’ history of crampy abdominal pain worsening over time. The pain was severe and diffuse in nature and non-responsive to high doses of analgesics. The pain increased in severity postprandially and was associated with intractable non-bloody diarrhea and weight loss of around 30 kg since the onset of his symptoms, but he had no fever or chills. The patient’s history is significant for a trauma laparotomy in April 2015 done in a field hospital for a blast injury that occurred in Syria. The patient suffered from multiple penetrating shrapnels that resulted in injury to the splenic flexure for which he underwent segmental resection and construction of a stoma, as well as an injury to the right lower extremity which resulted in a femur fracture that was stabilized using an external fixator device. The patient did well postoperatively and he underwent a re-laparotomy in July for stoma reversal. It was after the stoma reversal that the patient started developing the aforementioned symptoms that kept worsening until the time of presentation.
On presentation, the patient was noted to be weak and emaciated with basic investigations revealing anemia requiring blood products transfusion. As part of his work up a colonoscopy was done which revealed the healed anastomosis at 20 cm from the anal verge with the rest of the colonoscopy being normal. In view of the non-revealing colonoscopy a CT scan was done which showed dilated small bowel loops with dense heterogeneous material in the distal small bowel (Figure 1) raising the suspicion of a mass.
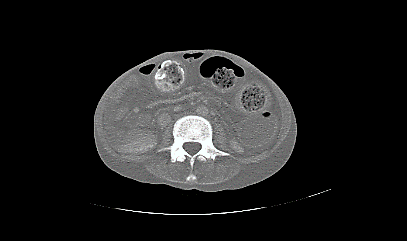
Figure 1: Axial cut CT scan with IV contrast showing small bowel dilatation and dense material in the lumen of the small bowel.
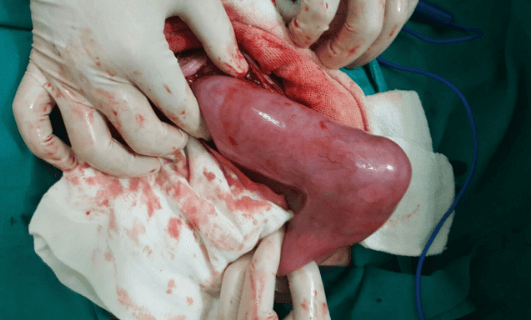
Figure 2: Intraoperative image showing a hard mass obstructing the small bowel.

Figure 3: Intraoperative image showing the Gossypiboma after the small bowel enterotomy was done.
The patient was taken to the operating room and he underwent an exploratory laparotomy with extensive release of adhesions. The small bowel was noted to have a hard mass within its lumen (Figure 2) therefore a small enterotomy was made overlying the mass (Figure 3) and a large pad was retrieved from the lumen (Figure 4). The enterotomy was closed primarily. The patient did well postoperatively, he was supported with peripheral nutrition until he regained normal bowel function by day 5 and was tolerating regular diet upon discharge. On follow up the patient was doing well and started regaining weight.

Figure 4: Intraoperative image showing the gossypiboma after complete retrieval from the small bowel.
Discussion
Retained surgical items (RSI) by definition is any item that was not intended to remain in a patient and is found after surgery, they can be surgical instruments, needles or sponges [8]. The likelihood of RSI was shown to be higher in rural hospitals compared to urban hospitals yet others associate emergency surgery and obesity with higher rates of RSI [9, 10]. The incidence of retained surgical pads also known as gossypiboma or textiloma is reported to be around 1 in 1000-1500 cases and they can have a spectrum of presentations [4]. They can present as intra-abdominal abscesses or intestinal fistulae or can remain asymptomatic for years and present later mimicking tumors or causing perforation or obstruction [5-7]. The natural history of a retained surgical pad is along the path of least resistance be it through the wound, or by forming a fistulous tract or by eroding into the lumen of a hollow viscous [11]. The possibility of intraluminal erosion as part of the body’s defense mechanism to isolate and extrude the foreign object is rare yet reported. It has been reported after C-section, hysterectomy and surgeries for acute abdomen and perforation [4, 12, 13].
The patients can initially have vague symptoms including malaise, abdominal cramps, fever or even incidental findings. This often leads to a delay in diagnosis ranging from 6 months up to 14 years in some chronic cases [14]. Our patient had initially vague symptoms that included crampy abdominal pain and diarrhea and the diagnosis was pinned few months after the onset when he had cachexia and the pain became more severe. Furthermore, it is crucial to highlight the fact that the incident occurred in a region that has been inflicted with war since 2011. The austere conditions under which the surgical staff in Syria and other war zones need to operate is often plagued with limited resources and minimal infrastructure [15]. Moreover, the indications to operate often include combat related and noncombat related indications with extreme constraints on follow up which can indirectly affect timely diagnosis, management and outcomes [15].
One outcome, RSI, as presented earlier can be reflective of the complex and intricate relationship that the patient has with a fragmented healthcare system and its implications. Notably, a higher incident of RSI has been reported during the Croatia war which presented mainly as intraabdominal masses [14]. To our knowledge our case is the first to report on small intestine intraluminal migration of a gossypiboma in trauma. The key is prevention of RSIs by meticulous surgical counts and the use of radiopaque surgical pads. Unfortunately, the surgical count was reported to be correct in 88% of cases of retained surgical instruments [10]. It is imperative to re-examine the abdominal cavity in select high risk operations even if the count was declared to be correct.
Conclusion
We conclude that the surgeon should be aware of the possibility of a retained surgical pad as part of the differential diagnosis of small bowel obstruction on a background of trauma laparotomy or major surgical procedures.
Consent
Consent to publish the case report was obtained from the patient. The consent was obtained over the phone since the patient resides in a different country. The report contains radiology image as well as intra-operative images without patient identifiers.
Funding
None.
Conflicts of Interest
None.
Abbreviations
Kg: Kilogram
CT: Computed Tomography
OR: Operating Room
SBO: Small Bowel Obstruction
POD: Postoperative Day
RSI: Retained Surgical Item
Article Info
Article Type
Case ReportPublication history
Received: Wed 22, Jul 2020Accepted: Sat 01, Aug 2020
Published: Fri 28, Aug 2020
Copyright
© 2023 Arwa El Rifai. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.08.14
Figures & Tables
References
- Jean-Jacques Duron, Nathalie Jourdan-Da Silva, Sophie Tezenas du Montcel, Anne Berger, Fabrice Muscari et al. (2006) Adhesive Postoperative Small Bowel Obstruction: Incidence and Risk Factors of Recurrence After Surgical Treatment: A Multicenter Prospective Study. Ann Surg 244: 750-757. [Crossref]
- Mehraneh D Jafari, Fariba Jafari, Jennifer E Foe-Paker, Michael J Phelan, Joseph C Carmichael et al. (2015) Adhesive Small Bowel Obstruction in the United States: Has Laparoscopy Made an Impact? Am Surg 81: 1028-1033. [Crossref]
- Michael L Kendrick (2009) Partial small bowel obstruction: clinical issues and recent technical advances. Abdom Imaging 34: 329-334. [Crossref]
- A Y Ukwenya, P M Dogo, A Ahmed, P T Nmadu (2006) The retained surgical sponge following laparotomy; forgotten at surgery, often forgotten at diagnosis. Our experience. Nigerian J Surg Res 8: 164-168.
- Roberts OA, Afuwape OO (2016) Intra‐abdominal gossypiboma with feacal fistula, laparotomy, removal and drainage. Trop J Obstet Gynaecol 33: 250‐253.
- Musa Atay, Issam Cheikh Ahmad, Mehmet Bilgin, Ercan Kocakoc (2014) Gossypiboma/textiloma mimicking as tumour recurrence. J Pak Med Assoc 64: 708-710. [Crossref]
- Evangelos Margonis, Dionysia Vasdeki, Alexandros Diamantis, Georgios Koukoulis, Grigorios Christodoulidis et al. (2016) Intestinal Obstruction and Ileocolic Fistula due to Intraluminal Migration of a Gossypiboma. Case Rep Surg 2016: 3258782. [Crossref]
- Gibbs V. NoThing Left Behind: a national surgical patient-safety project to prevent retained surgical items. New policies, practices and posters. Retained surgical items.
- Ahmad Elsharydah, Kimberly O Warmack, Abu Minhajuddin, Susan D Moffatt-Bruce (2016) Retained surgical items after abdominal and pelvic surgery: Incidence, trend and predictors- observational study. Ann Med Surg (Lond) 12: 60-64. [Crossref]
- Atul A Gawande, David M Studdert, E John Orav, Troyen A Brennan, Michael J Zinner (2003) Risk factors for retained instruments and sponges after surgery. N Engl J Med 348: 229-235. [Crossref]
- J W Hyslop, K I Maull (1982) Natural History of the Retained Surgical Sponge. South Med J 75: 657-660. [Crossref]
- Kundan K Patil, Shaifali K Patil, Kedar P Gorad, Anuradha H Panchal, Sahil S Arora et al. Intraluminal Migration of Surgical Sponge: Gossypiboma. Saudi J Gastroenterol 16: 221-222. [Crossref]
- Woo Young Shin, Chan Hyuk Im, Sun Keun Choi, Yun-Mee Choe, Kyung Rae Kim (2016) Transmural penetration of sigmoid colon and rectum by retained surgical sponge after hysterectomy. World J Gastroenterol 22: 3052-3055. [Crossref]
- Ratimira Klarić Custović, Ivan Krolo, Miljenko Marotti, Nenad Babić, Nikola Karapanda (2004) Retained Surgical Textilomas Occur More Often during War. Croat Med J 45: 422-426. [Crossref]
- Miguel Trelles, Lynette Dominguez, Katie Tayler-Smith, Katrin Kisswani, Alberto Zerboni et al. (2015) Providing surgery in a war-torn context: the Médecins Sans Frontières experience in Syria. Confl Health 9: 36. [Crossref]