Septic Tibial Shaft Non-Union Treated by One-Step Surgery Using a Custom-Made Intramedullary Antibiotic Cement-Coated Carbon Nail: Case Report, Focus on Surgical Technique and Brief Literature Review
A B S T R A C T
Septic non-union (SNU) represents an insidious complication of open fractures. SNU is defined as a clinical and radiological evidence of cessation of fracture healing after 6-8 months of treatment, associated with persistence of clinical, laboratoristic and radiological signs of infection. The infection is mostly caused by bacteria and when it occurs at the bone fracture site, the healing process slows down and generally the treatment takes place in multiple phases. First a surgical debridement, often with the use of polymethylmethacrylate and local antibiotics, associated with specific systemic antibiotic therapy and a temporary stabilization of the septic non-union. Once the infection is cleared up, the final definitive synthesis is performed. Recently the use of implantable antibiotic medical devices in one step surgery has been introduced with encouraging results and have shown numerous advantages both in terms of management and morbidity for the patient. There are several "pre-formed" devices on the market, which however must be approved by the institution and often have the limit of a high cost in addition to the impossibility of using specific antibiotics. We want to report our experience with a clinical case of a tibial SNU successfully treated by one-step surgery procedure using a custom-made intramedullary antibiotic cement-coated carbon nail. We focus on surgical technique, advantages and pitfalls related to the use of these devices.
Keywords
Septic non-union, carbon nail, open fractures, coated nail, tibial open fracture
Case Presentation
A 69-year-old man, affected by diabetes mellitus, in February 2021 suffered a left tibia open fracture (grade IIIB according to the Gustilo-Anderson classification) and multiple skin lacerated wounds associated with the lesion of Achilles tendon on the right leg (Figure 1) [1].
The patency of all three main vessels of the left leg was attested by an angiography carried out in the First Aid by vascular surgeons. The patient was then treated in emergency with a temporary External Fixation (EF), local debridement, irrigation, and systemic antibiotic prophylaxis according to the guidelines of open fractures (Cefazolin + Gentamicin). The soft tissue tears were subjected to debridement and skin suturing, while the Achilles tendon on the right leg was treated by direct tendon suture. After a few days it was necessary to modify the EF due to the presence of an extensive skin necrosis near the external malleolus, then treated with multiple surgical debridement, negative pressure therapy and at the end with covering skin flaps.
Later on, Enterobacter cloacae complex was identified in the wound cultural exams; the infectious disease specialist set antibiotic therapy with piperacillin/tazobactam associated with Fosfomycin, then modified with Linezolid and Levofloxacin, in the light of the improvement of the clinical status and inflammatory markers according to antibiogram. In April 2021 the patient underwent surgical toilette and reconstruction of the de-epithelialized areas at left leg with a Thiersch-type graft taken from the right thigh (Figure 2).
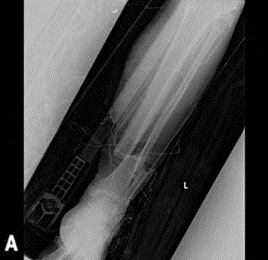
Figure 1: The Patient’s left tibia open fracture (grade IIIB according to the GustiIo-Anderson classification).
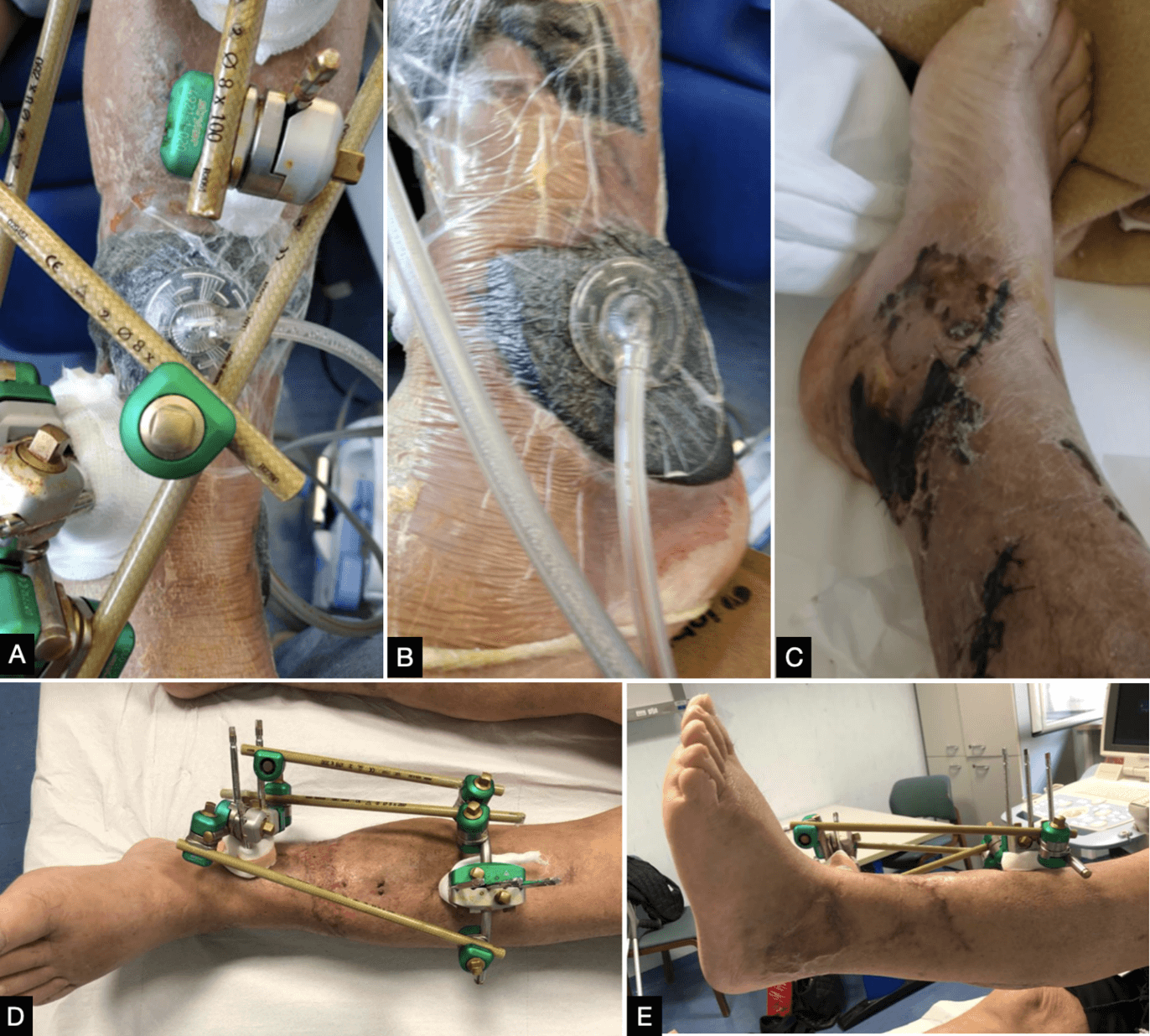
Figure 2: A & B) Negative pressure therapy applied over skin necrosis wounds respectively on the anterior aspect of the shinbone (A - previous exposure site) and on the lateral malleolus (B - skin necrosis area). C) Contralateral legs with skin necrosis area left to heal by secondary intention. D & E) left leg wound healing with flap engraftment a month after packing the Tiersch. External fixator has been left in place without changes to avoid flaps damage.
In June 2021 SPET was performed, and it didn’t show areas of pathological leukocyte accumulation in any site, neither in the fracture, nor near the synthesis with the EF. The patient continued to weightbearing on the affected leg without pain and local signs of infections (Figure 3).

Figure 3: A) Scintigraphy with no signal in the left leg. B-D) The patient walked with complete weightbearing on the affected leg, and he didn’t show any local signs of infection.
At 6 months the clinical and radiographic Follow-Up (FU) showed an exuberant callus with no signs of fracture consolidation and a bone stumps angulation in the sagittal plane. The appearance, moreover, of serum-purulent secretion from the screws of the external fixator, imposed its removal, the execution of samples for antimicrobial culture (then tested positive for Escherichia coli and taphylococcus aureus); a temporary cast was made, and the patient started a targeted antibiotic therapy for 21 days. After 15 days of wash-out from antibiotic therapy, the patient performed a new scintigraphy with marked leukocytes which showed a small cortical leukocyte accumulation in correspondence of the previous exposure area on the anterior aspect of tibial bone (Figure 4).

Figure 4: A) Scintigraphy with accumulation in the site of fracture exposure. B-C) X-rays at 6 months of follow-up. One can notice the absence of effective bone callus and an angulation at the fracture site both on B) coronal and C) sagittal planes.
In October 2021, due to the local condition and inflammatory markers normalization under antibiotic therapy, in agreement with the patient, exhausted by prolonged treatment and the consequent impairment of life activities, the tibial shaft non-union was treated by a one-step procedure with the implantation of a custom-made intramedullary carbon nail coated with antibiotic cement.
We used a CarboFix Tibial Nail (CarboFix Orthopaedics LTD, Herzliya, Israel) coated with Stryker Simplex P antibiotic cement with 1g of Tobramycin (Stryker Co., Kalamazoo, Michigan, USA) added with Amikacin powder 1g, under suggestion of an infection disease specialist. Both antibiotics were effective against isolated bacteria.
Surgical Procedure
The patient was positioned in supine position on the surgical table with the thigh on a dedicated support allowing to bend the knee over 90°. With the aid of intraoperative x-rays to detect the septic nonunion level, the stability of the fracture was tested. The tibial canal was progressively reamed by a trans-patellar incision in the proximal tibia until we reached a drilling diameter of 4 mm over the planned nail diameter.
The customized carbon nail was made separately on an instrument table in the same operative room using a medical sterilized silicone tube as a scaffold for the cement. The silicone tube had to be at least 2 mm in diameter wider than the nail, in order to have an antibiotic-coated cement coating of at least 1 mm all around the nail.
While one or two operators were approaching the surgery, another one with the instrumentalist prepared the customized nail on a sterile table apart. The selected sterile rubber tube was coated with sterile lubricant and filled with the cement added with the targeted antibiotic for isolated pathogen. So, the carbon nail was inserted into the silicon tube and placed into a basin full of physiological solution to cool the system down during the cement exothermic reaction, to avoid as far as possible antibiotics denaturation or alteration of the materials in use. Once the cement was solidified, the rubber scaffold was cut longitudinally with a scalpel and removed, obtaining a custom-made cement coated carbon nail. The nail holes for the screws were freed from the cement with a drill, the coated-nail surface was inspected in search of gaps that were not found, and the edges were smoothed to facilitate its insertion into the tibia.
Under intraoperative radiographic control, the nail was positioned by antegrade way using its own guidewire inside the tibial canal. The nail was fixed with 2 distal titanium screws, a fibula osteotomy was performed via lateral incision to allow compression of the tibial fracture, the fracture site was compressed and then the nail blocked with a proximal titanium screw. Surgical accesses were sutured, and x-rays checks were performed (Figure 5).
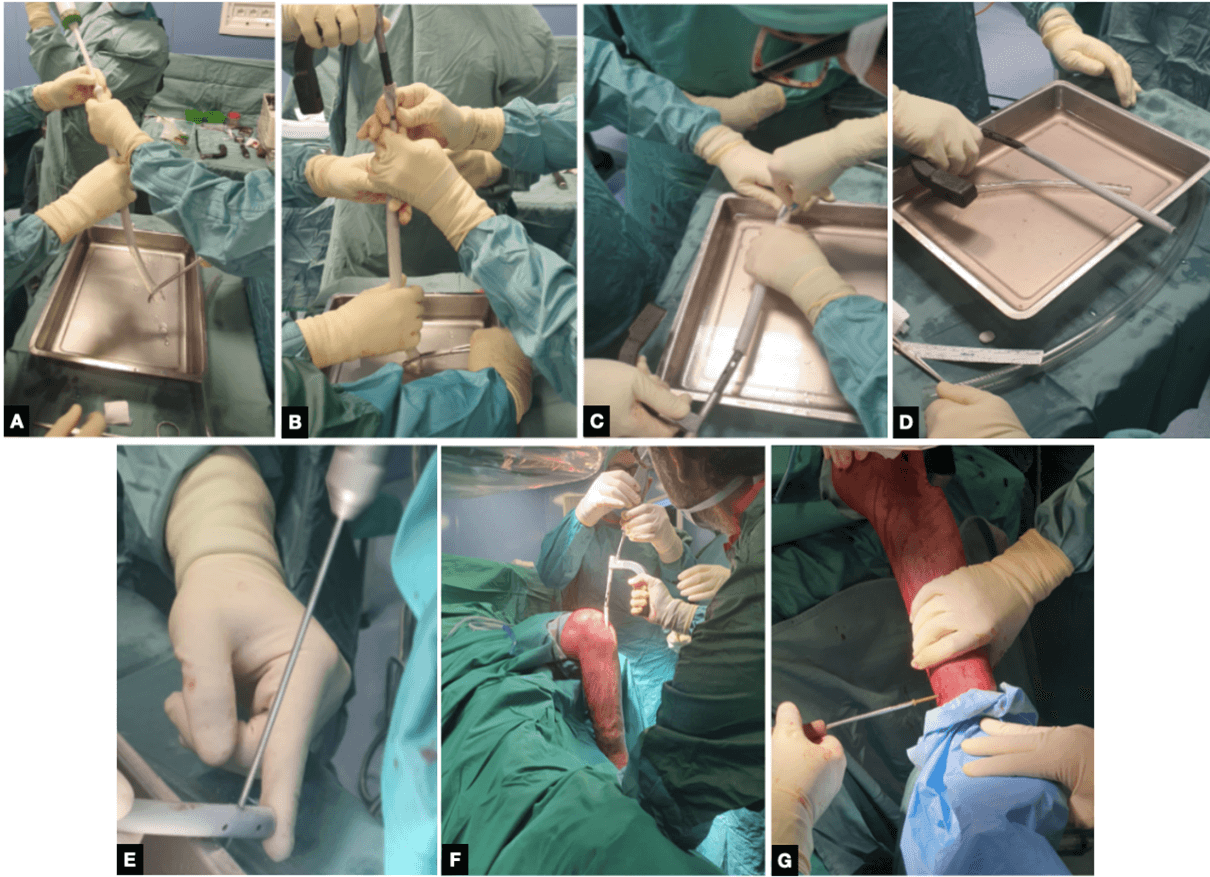
Figure 5: Surgical technique salient phases. A-E) carbon nail coating and preparation. F-G) Nail insertion and fixation. A) The rubber tube is prepared with medical sterile lubricant and clamped distally with a Rampley’s forceps to allow the cement insertion inside the scaffold. B) Nail insertion into the cement filled tube. C) The customized construct is then placed into a basin filled with saline solution to avoid antibiotic denaturation due to cement exothermic reaction and the scaffold tube is open longitudinally with a scalpel. D) The customized cement coated nail. One can notice the homogeneity of the coating. E) Before nail insertion the screw holes need to be pre-drilled to remove the exceeding cement. This operation has to be made carefully to avoid coating damage. F) The nail is then inserted into the tibial canal (previously reamed 4 mm wider than original nail diameter) through a trans-patellar approach. One can notice the patient's position with a support under the thigh to allow knee flexion. G) Nail fixation with screws throughout the pre-drilled holes.
During the surgery, multiple samples were taken for cultural tests which then gave negative results. After the surgery the weightbearing on the operated limb was granted in the immediate postoperative period and systemic antibiotic therapy was prolonged for 3 months until the scintigraphy (marked with leukocytes) and inflammatory markers normalized.
Tips and Tricks
The surgical technique seems to be not so challenging and with respect to the classical tibial nailing there is in addition “just” the “crafted” stage of the operation, but it's critical for the success of the intervention. The authors suggest considering a plan b, to check all the additional instruments before surgery (i.e., verify to have an adequate length of the basin and two or more rubber tubes with an adequate length and diameter based on nail length and diameter), to consider the final diameter of the coated-nail and consequently the additional reaming of tibial canal: in this regard when treating a “small” patient, an humeral nail can be used, due to its smaller standard diameters than tibial nails. Moreover, after drilling the screw holes of the coated nail before its insertion, it’s useful to position and remove a screw in the nail holes to be sure they were free from the cement and the screws can easily be positioned once the nail has been put in place.
Results
The patient underwent regular post-operative follow-up for up to 12 months post-operative. At the 6 months radiographic check, the formation of a mechanically and clinically satisfactory callus at the SNU site was observed (Figure 6). The patient achieved complete recovery of activity of daily living, normalization of the infection markers and complete recovery of the knee and ankle joint. There was no pain at the mobilization and load on the operated limb.
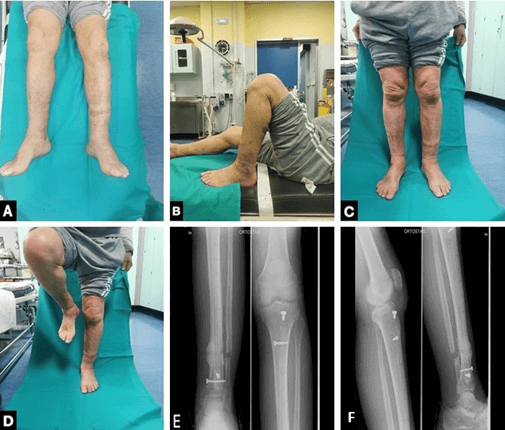
Figure 6: A-D) Clinical and E-F) radiological follow-up at 6 months. The patient was able to walk without crutches and without pain on his left lower limb. E) Radiological imaging demonstrates a certain callus formation and the distal screw breakage, that allowed additional local dynamization.
The scintigraphy took 6 months after surgery demonstrated the total disappearance of the pathological leukocyte accumulation in the tibial area and it has not been repeated due to the absence of clinical and laboratoristic signs of infection or pain (Figure 7).

Figure 7: A-B) Radiological and C-E) clinical one year follow-up. One can notice the progression of radiological callus and the complete clinical and functional restitutio ad integrum.
Discussion
In the orthopaedic and trauma fields, infections represent one of the most challenging complications to treat. The fixation or prosthetics devices represent an excellent substrate for the bacterial biofilms’ engraftment and proliferation, which are difficult to eradicate. In addition to this, they can represent a vector for the infection that can extend both to the bone and to the soft tissues, further complicating the possibility of fighting the infection itself in addition to the clinical picture [2, 3].
To overcome this complication, the two-step procedure has been the gold standard for prosthetic late-onset infection and for septic non-union treatment in recent years: the removal of the infected devices and the positioning of a polymethyl methacrylate spacer allows to administer to the patient an antibiotic therapy aimed at resolving the infection. Then, once the infection has been solved, a new surgical procedure with the removal of the spacer and final implant positioning can be performed [4].
Even if this approach has a good safety profile, on the other hand it implies a greater lapse of time between therapeutic steps and a dilation of the overall time for the resolution of the clinical picture. This scenario causes a great discomfort for the patient with consequences on his psycho-physical health as well as economic issues, multiple surgical steps results in a higher cost for the National Health System (NHS).
The one-step surgical approach allows, in selected cases, to optimize the effectiveness of local antibiotic therapy at high dosages, avoiding the side effects of a similar systemic therapy, and, at the same time, guaranteeing the stability of the fracture at the non-union level in the immediate post-operative time [5]. It results in an overall positive effect both for the patient's quality of life and for the NHS.
In the literature there are other cases in which septic non-union were treated with a one-step procedure with an antibiotic cement-coated intramedullary nail: Thonse and Conway reported a 95% success in controlling the infection on the 20 patients examined and the achievement of stability of fracture in 17 of these, with half of the patients requiring additional procedures to achieve infection control and fracture stability [6]. In their series these authors reported a heterogeneous population with multiple SNU sites treated. They used a titanium alloy nails and a metal bi-modular fold to coat the nails.
In another study Shyam et al. treated 23 femoral and 2 tibial septic non-unions using antibiotic-impregnated intramedullary nails after wide debridement; the goal of treating the infection and fracture stability was achieved in all patients with < 6 cm of bone loss [7]. These authors didn’t specify which kind of nails they used and applied the cement coating with a free hand technique without the use of a scaffold.
In a previous publication we reported a femoral shaft septic non-union successfully treated by one step surgery with a customized cement coated carbon nail, reporting economic advantages and a gain in the patient’s quality of life gain [8]. Also, in this case we used a similar surgical technique as the one described above in the text.
In literature we found studies that show how the treatment with antibiotic-coated nail represents a valid option in case of open fractures non-union: the 2015 report of W. J. Metsemakers et al. shows the efficacy of commercial gentamicin-coated nail in preventing deep infection in most of type 2-3 tibia open fracture [9].
Rachel M. Reilly et al. considered their group of 31 patients who underwent a second surgery with an antibiotic intramedullary nail as treatment of deep infection after an open fracture: 76% of infections were cleared at the 6-month time frame, showing that the use of antibiotic nails for treatment of tibial infections seems to be a reasonable therapeutic option [10].
In the last two cited case series, the authors utilized a commercial pre-formed antibiotic impregnated nail without targeted antibiotics against the isolated bacteria. Their clinical results were remarkable in treating the infection. The commercial pre-formed coated nails present several benefits: there are specific data published about time and quantity of antibiotics release at SNU site (from 2 weeks up to 6 months after the implant positioning), they are ready to use and there are no risk of coating debonding during nail insertion or removal. On the other hand, they have a higher cost than standard nail, there isn’t the possibility to add specific targeted antibiotics and often they have to be acquired by the institution under specific request.
In the custom-made cement-coated nails was impossible to rate the impact of the cement exothermic reaction on the denaturation of the added antibiotics and consequently the effective quantity that has been implanted and then released over the time at SNU sites. This aspect represents the main disadvantages of custom-made nails. Other disadvantages are represented by the complex surgical preparation with its pitfalls and the risk of coating debonding during nail insertion or removal [6].
In literature we found a meta-analysis that shows that antibiotic loaded bone cements can release antibiotics, even if dose efficiency is low [11]. The cited studies show a common initial burst, and then a rapid decay in the elution rate for the antibiotics. Moreover, the thickness of the cement and the concentration of the added antibiotic are proved to influence the release rate and the polymerization of the cement also can contribute to increasing or lowering the antibiotic elution through the construct [12, 13].
Our case report differs from the cited works in several aspects: we used a carbon nail and another surgical technique to package the bone-cement coating. Respect to the case series reports by Thones et al. and Shyam et al. we consider that the use of single-use sterile medical silicon tube as scaffold can be advantageous over the use of bi-modular metal scaffolds or free hand technique: the perfect circular smooth internal surface of the tube allow to obtain a more homogenous cement coating distribution over the nail and the simple scaffold removal by cutting the tube allows not to damage the coating and this could prevent from coating itself debonding [6, 7]. On the other hand, the impact of the cited works is remarkable: in both publications are reported several cases pioneering treaded with success in a custom-made manner. Thones et al. treated several heterogeneous complex cases, while Shyam et al. reported cases with wide bone defects and give important indications about the cut-off of defects and clinical outcomes.
However, in our experience the use of a carbon nail represents an innovative solution in comparison to other cases: the ordinary titanium alloy made nails causes artifacts at the CT and MR imaging. It can make difficult the bone healing or other complications evaluation during the follow-up. In addition, carbon fiber constructs have an elastic modularity more like bone cortex than titanium: it can improve the resistance to mechanical stress and bring to a faster recovery [14, 15].
No complications have been reported in the literature as we know, probably due to the sporadic use of this kind of device, with the exception of the cited coating debonding, which could cause intraoperative difficulties and medico-legal issues. Moreover, the SNU non-healing could be attributed to the tampering of the device in the medical examiner's office in the event of a dispute for the pseudoarthrosis non-healing. However, even if not corroborated by official data, this treatment is taking place with good results as shown by the data in the literature which in any case have their weight in the medical examiner. The authors, however, suggest preparing dedicated informed consents specifying the experimental nature of the surgery.
More extensive and detailed reports could be published in the future to definitively validate the efficiency of the procedure. Moreover, our article providing in detail all the procedural phases could allow other colleagues to conform to our technique in order to reach a larger number of cases with the same surgical technique and provide data for multicentric analysis.
Conclusion
In our experience, the use of the custom-made carbon nail coated with antibiotic cement has proved to be the winning choice to bring the patient to a rapid recovery from the infection (by conveying the target antibiotic for the isolated microorganism through the cement), to a faster return to the activity of daily living and to guarantee the stability and elasticity to septic non-union site. All this guarantees both the patient and the sanitary system lower economic and temporal costs, with a full recovery of autonomy and quality of life in the shortest time, also avoiding as far as possible antibiotics side effects.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Mon 31, Oct 2022Accepted: Mon 14, Nov 2022
Published: Thu 09, Feb 2023
Copyright
© 2023 Giuntoli Michele. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2022.11.06
Figures & Tables
References
1. Gustilo RB, Mendoza
RM, Williams DN (1984) Problems in the management of type III (severe) open
fractures: a new classification of type III open fractures. J Trauma 24:
742-746. [Crossref]
2. Patzakis and
Zalavras, 2005; Patzakis et al., 1986; Barger et al., 2017; Chadayam- muri et
al., 2017; Beals and Bryant, 2005.
3. Barger et al.,
2017; Koury et al., 2017; Paley and Herzenberg, 2002; Bhadra and Roberts, 2009.
4. Romanò CL, Romanò
D, Meani E, Logoluso N, Drago L (2011) Two-stage revision surgery with
preformed spacers and cementless implants for septic hip arthritis: a
prospective, non-randomized cohort study. BMC Infect Dis 11: 129. [Crossref]
5. Nizegorodcew T,
Palmieri G, Marzetti E (2011) Antibiotic-coated nails in orthopedic and trauma
surgery: state of the art. Int J Immunopathol Pharmacol 24: 125-128. [Crossref]
6. Thonse R, Conway J
(2007) Antibiotic cement-coated interlocking nail for the treatment of infected
nonunions and segmental bone defects. J Orthop Trauma 21: 258-268. [Crossref]
7. Shyam AK, Sancheti
PK, Patel SK, Rocha S, Pradhan C et al. (2009) Use of antibiotic
cement-impregnated intramedullary nail in treatment of infected non-union of
long bones. Indian J Orthop 43: 396-402. [Crossref]
8. Bonicoli E,
Piolanti N, Giuntoli M, Polloni S, Scaglione M (2020) Septic femoral shaft
non-union treated by one-step surgery using a custom-made intramedullary
antibiotic cement-coated carbon nail: case report and focus on surgical
technique. Acta Biomed 91: e2020176. [Crossref]
9. Metsemakers WJ,
Reul M, Nijs S (2015) The use of gentamicin-coated nails in complex open tibia
fracture and revision cases: A retrospective analysis of a single centre case
series and review of the literature. Injury 46: 2433-2437. [Crossref]
10. Reilly RM,
Robertson T, O'Toole RV, Manson TT (2016) Are antibiotic nails effective in the
treatment of infected tibial fractures? Injury 47: 2809-2815. [Crossref]
11. Mensah LM, Love BJ
(2021) A meta-analysis of bone cement mediated antibiotic release: Overkill,
but a viable approach to eradicate osteomyelitis and other infections tied to
open procedures. Mater Sci Eng C Mater Biol Appl 123: 111999. [Crossref]
12. Gandomkarzadeh M, Mahboubi A, Moghimi HR (2020) Release behavior, mechanical
properties, and antibacterial activity of ciprofloxacin-loaded acrylic bone
cement: a mechanistic study. Drug Dev Ind Pharm 46: 1209-1218. [Crossref]
13. Sundblad J, Nixon
M, Jackson N, Vaidya R, Markel D (2018) Altering polymerization temperature of
antibiotic-laden cement can increase porosity and subsequent antibiotic
elution. Int Orthop 42: 2627-2632. [Crossref]
14. Hak DJ, Mauffrey C, Seligson D, Lindeque B (2014) Use of carbon-fiber-reinforced composite implants in orthopedic surgery. Orthopedics 37: 825-830. [Crossref]
15. Pala E, Procura A, Trovarelli G, Berizzi A, Ruggieri P (2022) Intramedullary nailing for impending or pathologic fracture of the long bone: titanium vs carbon fiber peek nailing. EFORT Open Rev 7: 611-617. [Crossref]