Retained Metallic Part of a Dislodged Knife in the Thoracic Spine with Paraparesis
A B S T R A C T
The incidence of traumatic spinal cord injury is reported as 30-40 million per year. Among these, stab wounds to the spinal canal are usually rare. These injuries often lead to complete or incomplete neurological deficits. An appropriate management can ensure good functional recovery for approximately two-third of the patient. As these cases are uncommon, their treatment protocols are still controversial and under evaluation. Some literatures reveal various surgical approaches. Spinal canal injury with retained part of the causative agent (knife, bullet, glass etc.) or any other complication on the wound site demands immediate surgical exploration. Here we report on a patient with a retained metallic foreign body (tip of knife) in the thoracic region traversing the left pedicle of sixth thoracic vertebrae along with spinal canal with paraparesis and after neuro-surgical exploration and complete removal of the foreign body, patient shows gradual improvement of neuro-functional status. Proper wound care and long term close follow up was ensured during post operative period.
Keywords
Thoracic spine, retained metallic part, paraparesis, penetrating spinal injury, laminectomy
Introduction
Spinal cord injuries reported all over the world are presented with different aetiologies, which includes motor bike accident, fall from height, firearm injury, fall of heavy weight on back, soft tissue injury and stab. After trauma, retained bullets, glass fragments, knife blades or broken bony parts frequently injure the spinal cord. Thoracic region is the most common site for non-missile penetrating injury, which is explained by the defensive position of the victim during attack [1]. In earlier period, some retained products don`t cause any neurological deficit, but in the long run, some may contribute to new symptoms. The foreign bodies can enter the spinal canal via intra-laminar space or intra-vertebral foramen and sometimes can be lodged in the vertebral bodies (lamina, pedicle) [2]. Along with conservative treatment, surgical exploration is strongly suggested for spinal stab wounds if there is any retained part [3]. Such patient with immediately apparent complications such as excessive bleeding, CSF leakage or any neurological deficit deserves urgent response. Optimal treatment strategy remains challenging and should be assessed case by case [2].
Localization of the foreign body must be specific by using X-ray, ultrasound, computed tomography or magnetic resonance imaging. After localizing the most probable site, careful positioning(prone), meticulous dissection, surgical dissection by laminectomy, haemostasis and complete extraction of the FB(Foreign Body) in the original trajectory path and management of dural injury should be ensured [1, 4]. On post operative period, prevention of infection, careful neurological evaluation, regular follow up of the patient has paramount importance for less complication and fast recovery [5, 6].
Case Report
A 32-year-old male patient presented with pain in mid back region with progressive paraparesis (left>right) with stab injury with retained foreign body 04 months back. Then he underwent emergency exploration, and a single large metallic part of the stabbing knife was removed. In post-operative period, X-ray and CT scan reveals a retained FB (tip of knife), traversing the left pedicle of D6 involving the spinal canal (Figures 1-3).
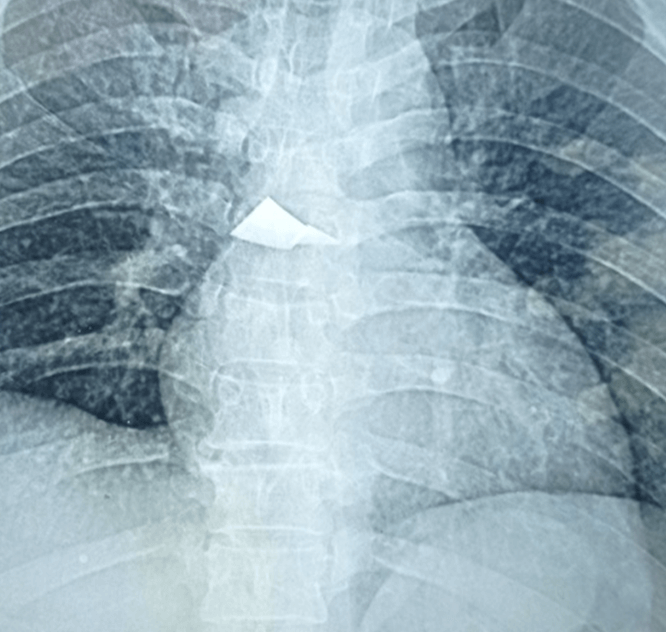
Figure 1: Plain X-ray chest showing a radio-opaque shadow of the retained two metallic pieces of the tip of the knife.
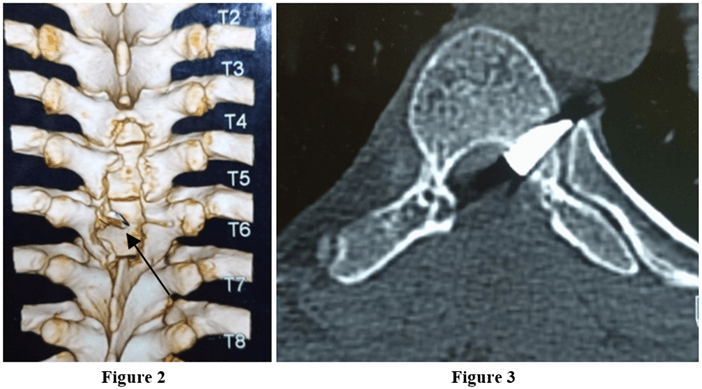
Figures 2 & 3: CT scan of dorsal spine with 3D reconstruction shows a hyper-dense shadow of retained triangular shaped foreign body traversing the left pedicle of D6.
Later on, he developed post-surgical discharging sinus from wound site. Neurological examination reveals ‘Brown Sequard syndrome’ with MRS grading 2/5 on left lower limb. After second look operation with Left Hemi-laminectomy, FB was found in the spinal canal traversing left pedicle of D6 (Figure 4). After meticulous sub-periosteal dissection avoiding any injury to pleura, dura or spinal cord, subsequent drilling was done to explore the affected area and ensure the complete extraction of all remaining fragments of metallic tip (which consisted of three pieces) (Figure 5). Then the wound was carefully inspected for bleeding or CSF leakage. Wound was meticulously cleansed with anti-septic solution and normal saline. Immediately after operation his neurological examination was gradually improving with healthy wound. Post operative radio imaging (X-ray) shows no residue of foreign body (Figure 6).
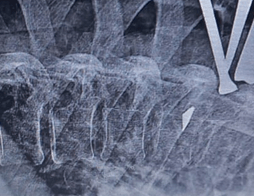
Figure 4: Intraoperative X-ray showing the radio-opaque shadow of the foreign body.
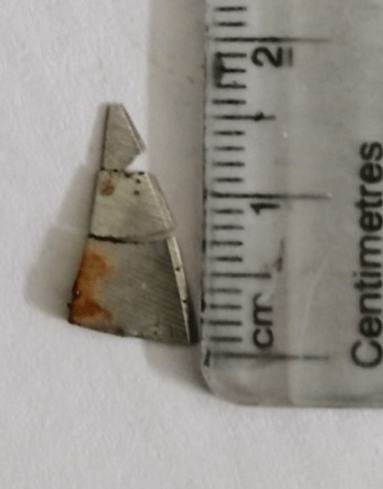
Figure 5: The figure shows total three pieces of the retained tip of the knife measuring about 1.5cm in length.

Figure 6: Postoperative X-ray of dorsal spine shows no retained foreign body.
We treated him with broad spectrum antibiotics and other supportive measures. He was discharged after 10 days and was advised for regular follow up at every 2 months interval.
Discussion
Spinal stab wounds are commonly found in the thoracic region and comparatively less in cervical and lumbar area. The biomechanical structure of thoracic vertebrae is very stable as there are costo-vertebral joints and thoracic cage. Although any injury to this area demands much force, as the thoracic spinal canal is narrower than the rest of the spinal zone, this region is more prone to damage [7]. Furthermore, the caudal half of the spinal cord is supplied by the “Artery of Adamkiewicz”, located in the inferior thoracic zone, can be rooted in any segmental artery in between T6-L3 [8]. As a result, the powerful thrush made by a metallic knife can cause multiple different injuries to the thoracic zone, which can threat the primary nourishment of the spinal cord [5].
Following a stab injury, direct damage to the spinal cord can be caused by weapon itself, any metallic particle or due to compression of the broken bone particles/injured disc material. the peculiarity of the case presented here is that the broken tip of the dislodged knife is settled in the middle thoracic zone (2 pieces). In the first attempt of the removal in other hospital, the larger one was extracted, but the smaller one was impacted in the left pedicle of the D6 and while traversing, which caused bony defect and paraparesis. Certain historical factors, we should consider about a retained FB, the mechanism of the injury, composition and shape of the wounding object, and the type and location of the resulting wound [9]. A sharp, well localized pain with tenderness on palpation over a puncture wound is a very useful sign.
The most common retained FB is “Glass”, and it is always difficult to diagnose [7, 9]. Any retained FB can cause delayed healing, pain, nerve laceration and tissue infection [8]. As our patient presented late (approximately after four months), we did complete neurological examination, special attention to the late symptoms of neurological worsening-such as backache, cauda equina symptoms and radiculopathy, which can be a result of chronic inflammation and fibrous tissue formation around metallic particle [1].
The incidence of spinal stab injury is less, but the percentage of neurological deficit is high [10]. There are three modes of this injury: i) Direct injury to the spinal cord, ii) Incomplete injury (Brown-Sequard syndrome), iii) Complete injuries [11]. The very first complaint of spinal cord injury is “Pain” [5]. The other mechanisms of the cord damage include insult to the vascular supply of the spinal cord, edema, hemorrhage, ischaemia of the spinal cord and countercoup contusion. To avoid the secondary damage, an immediate short course of intravenous “Methylprednisolone” is recommended for reducing cellular damage, which was not given in our case due to delayed presentation.
The routine X-Ray studies are cheap, effective and easily available modality to detect most of the FBs. If plain radiograph cannot reveal, then Fluoroscopy, Ultrasound (US) and Computed Tomography (CT scan) of the affected zone are usually recommended [11, 12]. CT scan is a preferred study in the emergency department because it provides information of spinal stability, wound trajectory, bone injury and involvement of vital structures [1]. Whereas, Magnetic Resonance Imaging (MRI) is very useful for diagnosis of spinal cord injuries, because it provides a superior view of the extent of the injury, including path of the blade, intra-spinal hemorrhage, acute cord edema and contusion [7, 8]. But it is a “MUST” concern that, if history/X-ray confirms that, there is a retained particle, MRI is contraindicated and must be avoided due to the risk of mobilization and heating of the material to prevent the secondary damage to the spinal cord and surrounding tissues [12-14].
Retained foreign bodies as needles and wires can possibly migrate into the spinal canal over time and can cause nerve injuries [15]. In the long run, when neural elements on wound site are no longer capable of adjusting the new changes, retained FB can cause some local reaction that leads to neurological deficits and demands surgical removal [16]. In some failed surgical attempts, the foreign fragment remains with no grievous complaints and thus regular follow-up appointments is advised [17]. The “Spring Phenomenon” says the long-lasting FB could penetrate into the intra-dural space, gradually close to the cord and nerve roots [18]. Sometimes in Para- vertebral soft tissues and extra-medullary space, pieces of surgical equipments can retain which mimics with neoplasm [19]. In case of acute penetrating injury or suspected metallic FB, CT and Radiographs are considered to be a safe option [19].
To avoid the time wastage and further injury, accurate localization of the FB should be ensured by C-arm- X-ray before surgical approach. In our patient, the pre-operative imaging helped us to detect the exact location and surgical approach was adequately planned for successful removal [4]. After complete removal, all three metallic parts combinedly completes the shape of the tip of the knife.
The surgical approach is always challenging to remove the FB, buried deep in the soft tissue [3]. Any possibility of vessel or nerve injury, persistent CSF leakage, radiologic signs of cord compression and infection in delayed stage are the indications of surgical exploration to remove the retained FB to prevent infection, myelopathy and delayed neurological deficit [20]. Some recommendations suggest surgical exploration even when imaging shows no retained product, but most of the case reports describing spinal stab wounds propose surgical procedure to extract the lodged part/weapon [14, 21, 22]. As the location of the FB varies from patient to patient, there is no ideal/universal procedure till date, but the described ones are-Exploration to the level of the lamina, laminectomy at the level of the lamina, laminectomy at the upper and lower lamina, lateral exposures and so on. In case of penetrating spinal cord injury, laminectomy is usually indicated for complete removal of the foreign body to prevent delayed presentation and persistent contamination [2]. Here we did the Hemilaminectomy in T5-7.
Undoubtedly, complete/incomplete nerve injury and if there is a retained foreign body due to a stab wound, surgical exploration is must, to ensure adequate decompression of the cord and to reduce the possibility of secondary/late injury [3]. There is no available data concerning neurological outcomes of those patients suffering from different spinal stab wounds. The associated risk factors of surgical exploration of the wound are enlarging the incision, muscle dissection, enlarging dural tear, removal of the lamina/other bony elements which may leads to instability in the long run.
Conclusion
Retained part of metallic foreign body lodged in spinal canal should be explored under proper guidance of X-Ray/CT scan. Proper pre-operative imaging evaluation is ensured during removal of any metallic FB. Otherwise, part of FB may be retained. Patient presented with any retained FB with neurological deficit is an obvious indication for surgical approach to improve neuro-functional status and to prevent further damages. Early surgical intervention must be ensured. After surveying the literature, we reported the unusual occurrence of retained metallic part of a dislodged knife in thoracic spine as observed in this case.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Fri 23, Sep 2022Accepted: Thu 06, Oct 2022
Published: Thu 20, Oct 2022
Copyright
© 2023 Fateha Yasmin Antara. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2022.10.04
Figures & Tables
References
1. Castillo Amaya C,
Prieto Meré JA, Cobar Bustamante A, Herrera Ovalle RM, Alonzo F (2021) Stab
injury to the spine without neurological involvement: a report of a rare case. J
Surg Case Rep 2021: rjab163. [Crossref]
2. Zhang P, Liu X,
Zhou D, Zhang Q (2022) Laminectomy for Penetrating Spinal Cord Injury with
Retained Foreign Bodies. Orthop Surg 14: 1476-1481. [Crossref]
3. Sakar M, Dogrul R,
Niftaliyev S, Bayri Y, Dagcınar A (2016) Direct withdrawal of a knife lodged in
the thoracic spinal canal in a patient with normal neurologic examination: is
it safe? Spinal Cord Ser Cases 2: 16009. [Crossref]
4. Ozsarac M, Demircan
A, Sener S (2011) Glass foreign body in soft tissue: possibility of high
morbidity due to delayed migration. J Emerg Med 41: e125-e128. [Crossref]
5. Kalkan E, Keskin F,
Cengiz ŞL, Baysefer A (2007) A case report of firearm bullet settling into the
thoracic spinal canal without causing neurological deficit or vertebral bone
destruction. Arch Orthop Trauma Surg 127: 637-641. [Crossref]
6. Waters RL, Sie I,
Adkins RH, Yakura JS (1995) Motor recovery following spinal cord injury caused
by stab wounds: a multicenter study. Paraplegia 33: 98-101. [Crossref]
7. Turner J, Wilde CH,
Hughes KC, Meilstrup JW, Manders EK (1997) Ultrasound-guided retrieval of small
foreign objects in subcutaneous tissue. Ann Emerg Med 29: 731-734. [Crossref]
8. Jacobsohn M, Semple
P, Dunn R, Candy S (2007) Stab injuries to the spinal cord: a retrospective
study on clinical findings and magnetic resonance imaging changes. Neurosurgery
61: 1262-1267. [Crossref]
9. Kaiser CW, Slowick
T, Spurling KP, Friedman S (1997) Retained foreign bodies. J Trauma 43:
107-111. [Crossref]
10. Van den Berg ME,
Castellote JM, Mahillo Fernandez I, de Pedro Cuesta J (2010) Incidence of
spinal cord injury worldwide: a systematic review. Neuroepidemiology 34:
184-192. [Crossref]
11. Arbona N,
Jedrzynski M, Frankfather R, Lo AE, Hetman J et al. (1999) Is glass visible on
plain radiographs? A cadaver study. J Foot Ankle Surg 38: 264-270. [Crossref]
12. Graham Jr DD (2002)
Ultrasound in the emergency department: detection of wooden foreign bodies in
the soft tissues. J Emerg Med 22: 75-79. [Crossref]
13. Shahlaie K, Chang
DJ, Anderson JT (2006) Nonmissile penetrating spinal injury: case report and
review of the literature. J Neurosurg Spine 4: 400-408. [Crossref]
14. Xia X, Zhang F, Lu
F, Jiang J, Wang L et al. (2012) Stab wound with lodged knife tip causing
spinal cord and vertebral artery injuries: case report and literature review. Spine
37: E931-E934. [Crossref]
15. Yoshioka K,
Kawahara N, Murakami H, Demura S, Matsuda M et al. (2012) A glass foreign body
migrating into the lumbar spinal canal: a case report. J Orthop Surg 20:
257-259. [Crossref]
16. Wu WQ (1986)
Delayed effects from retained foreign bodies in the spine and spine cord. Surg
Neurol 25: 214-218. [Crossref]
17. Lv X, Lu X, Wang Y
(2018) Entrapment of a metal foreign body in the cervical spinal canal during
surgical procedure: A case report. Medicine 97: e0548. [Crossref]
18. Li H, Lou J, Liu H
(2016) Migration of titanium cable into spinal cord and spontaneous C2 and C3
fusion: case report of possible causes of fatigue failure after posterior
atlantoaxial fixation. Medicine 95: e5744. [Crossref]
19. Reddy N, Fata P,
Balzer A, Diaz Marchan P, Lincoln CM (2017) Thorn in My Spine: A case of a
retained intradural extramedullary foreign body. Clin Imaging 45:
118-121. [Crossref]
20. Williams DT, Chang
DL, DeClerck MP (2009) Penetrating spinal cord injuries with retained canal
fragments. CJEM 11: 172-173. [Crossref]
21. Rubin G, Tallman D, Sagan L, Melgar M (2001) An unusual stab wound of the cervical spinal cord: a case report. Spine 26: 444-447. [Crossref]
22. Li X, Curry EJ, Blais M, Ma R, Sungarian AS (2012) Intraspinal penetrating stab injury to the middle thoracic spinal cord with no neurologic deficit. Orthopedics 35: e770-e773. [Crossref]