Repair of Ruptured Sinus of Valsalva Aneurysm: Rare Cause of Acute Onset Congestive Heart Failure in Down’s Syndrome
A B S T R A C T
A 20-year-old boy with Down´s syndrome presented to the emergency department with new onset acute heart failure. Right side chest effusion and cardiomegaly was observed on chest x-ray. A mobile aneurysmal sac protruding into the right atrium was detected and a ruptured aneurysm of the right coronary sinus of Valsalva was observed in transthoracic echocardiogram. Cardiac angiography catheterization confirmed the diagnosis. Surgical repair consisting of aneurysm resection and defect closure was performed shortly after with pericardium reinforced suture through the right atrium. The patient was discharged uneventfully.
Keywords
Congenital heart disease, Aneurysm, heart failure, congenital heart surgery
Introduction
Aneurysm of one of the aortic sinuses of Valsalva are rare lesions, which may be congenital or acquired. The dilated sinus may bulge into one of the cardiac chambers; the most feared complication is a sudden catastrophic rupture of the aneurysm. Owing to their clinical silence, unruptured aneurysms remain either undiagnosed or become corrected before rupture [1]. We report an unique case of a boy with Down syndrome and sudden rupture of sinus of Valsalva aneurysm, with normal aortic sinuses in infancy.
Material and Methods
A 20-year-old boy suffering from Down´s syndrome presented to the emergency department complaining of progressive shortness of breath and chest pain since one month previously. He has had no previous history of congenital heart disease. On physical examination he showed sinus tachycardia, his blood pressure was 110/56 mm Hg and his peripheral saturation breathing room air was 96%. A 3/6 continuous, blowing and high pitch murmur was auscultated on the mesocardium area. A chest x-ray showed cardiomegaly and significant right pleural effusion.
A transthoracic echocardiogram revealed mildly decreased left ventricular ejection fraction, competent auriculoventricular valves, moderate size circumferential pericardial effusion without signs of cardiac tamponade. A big mobile aneurysmal sac protruding into the right atrium (RA) was detected and a ruptured aneurysm of the right coronary sinus of Valsalva was suspected. Echocardiographic colour flow Doppler confirmed continuous flow between the aneurysmal sinus and right atrium (Figures 1A-1C). A cardiac catheterization revealed a competent aortic valve and the aneurysm originating from the right coronary cusp of the valve protruding and draining into the RA adjacent to the tricuspid valve (Figure 1D).
Surgical repair was performed subsequently. After sternotomy 1500ml of serous fluid were drained from the right pleura and pericardium cavity. The RA was severely dilated, and a thrill palpated. After cardiopulmonary bypass and aortic cross clamp, transverse aortotomy was carried-out at the root to deliver antegrade cardioplegia through both coronary ostium. Through right atriotomy (Figure 1E), a “windsock” aneurysm of the right coronary sinus (20 mm x 15 mm) was observed protruding into the RA, immediately above the tricuspid valve plane, with two 5 mm perforations at the end. After aneurysm resection, the 5 mm fistulous tract was closed with a double running autologous pericardium pledgeted 4-0 prolene suture (Figures 1F-1G). After aortic and atrium closure was achieved, the cross clamp was removed, the patient recovered sinus rhythm and was weaned off from cardiopulmonary bypass uneventfully.
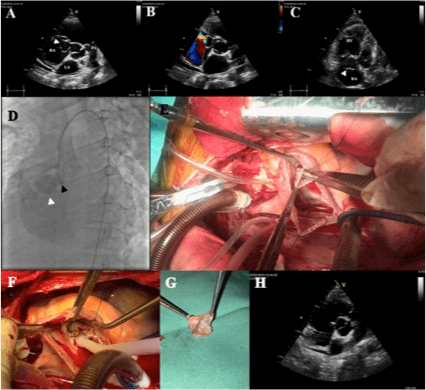
Figure 1: A) Transthoracic echocardiogram. Parasternal short axis view: aneurysmatic sac (white arrow) in the right atrium below the tricuspid valve. B) Parasternal short axis view: color Doppler flow from the aneurysm sac to the right atrium. C) Four apical chambers view with focus on the right ventricle: dilated right ventricle and aneurysm sac (white arrow) below the tricuspid valve. D) Aortogram: deformation of the right coronary cusp (black arrow) with the aneurysmatic sac (white arrow) filled by contrast revealing flow into the right ventricle. Also a closed aortic valve is seen with no incompetence. E) Intraoperative photograph of ruptured aneurysm of the right sinus of Valsalva with a "windsock" morphology, seen through a right atriotomy (forceps inside the sac). F) Surgical view after surgical closure of fistulous tract with doble layer prolene suture. G) Ruptured aneurysm sac resected. H) Follow-up transthoracic echocardiogram picture with the sinus of Valsalva repaired.
Results and Discussion
Follow up transthoracic echocardiogram revealed no residual leak and trivial aortic regurgitation. All three aortic sinuses have normal appearance. The patient was discharged at day 5 postoperatory in good conditions. Sinus of Valsalva aneurysm (SVA) is a rare disease that has an incidence of 0.14%-0.23% in Western series. The right coronary cusp is most affected (65%-86%) and most commonly rupture into the right ventricle (75%) [2, 3]. Most cases remain asymptomatic but symptoms such as acute dyspnea, chest pain and heart failure may arise if the aneurysm ruptures [4]. Cardiovascular anomalies are found in 40-50% of children with Down syndrome, the most common being septal defects and tetralogy of Fallot. Few cases have been reported of SVA rupture in patients with Down’s syndrome [1, 4-6].
Congenital aneurysms are caused by weakness at the juncture of the aortic media and the annulus fibrosus and a finger-like aneurysmal sac develops as a result of the weakened tissue and prolonged exposure to high aortic pressures. Endocarditis, chest trauma, or strenuous physical activity may result in further weakening of the thinned wall, eventually leading to rupture of the aneurysm. The most common site of rupture is into the RA, like our reported case [1, 5].
Surgical repair of a ruptured SVA has excellent outcomes, minimal risk for recurrent aneurysm formation and a small risk for aortic insufficiency later in life. The primary goals of surgical repair of SVAs are to close the aneurysm without distorting the aortic sinus, remove the aneurysmal sac, correct any associated intracardiac abnormalities, and prevent residual AR. The dual approach (both right atrium and aortic sides) has been reported as the best and most frequent approach. Methods for the surgical repair of SVA includes primary suture or patch closure [7]. Our dual approach surgical repair with autologous pericardium reinforced running suture was effective and easy to perform. SVA is rare and in association with Down syndrome extremely infrequent. We report the case of a patient with this extremely unique association of Down syndrome and acute rupture of SVA with congestive heart failure successfully treated at our institution.
Disclosure
None.
Consent
Permission was granted by the patient and family to publish this report.
Article Info
Article Type
Research ArticlePublication history
Received: Wed 03, Jun 2020Accepted: Tue 16, Jun 2020
Published: Mon 22, Jun 2020
Copyright
© 2023 Ignacio Juaneda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JICOA.2020.03.10
Figures & Tables
References
- Najim Lahrouchi, Lukas A J Rammeloo, David R Koolbergen, Jaroslav Hruda (2014) Ruptured aneurysm of the right coronary sinus of Valsalva in a child with Down syndrome. Cardiol Young 24: 376-378. [Crossref]
- Pei-Chun McGregor, Yutthapong Temtanakitpaisan, Aimee Hiltbolt, Jayashri R Aragam (2017) A spectrum of sinus of Valsalva aneurysm- From the young to the old. Echocardiography 34: 1524-1530. [Crossref]
- Xiaokang Luo, Dong Zhang, Bo Li, Lei Qi, Li Gong et al. (2019) Surgical repair of a ruptured congenital sinus of Valsalva aneurysm: 10-year experience with 286 cases. Eur J Cardiothorac Surg 55: 1211-1218. [Crossref]
- Rebecca Napier, Jonathan D Gardner, Susan Noe, Joe B Calkins Jr (2015) A continuous cardiac murmur. Cleve Clin J Med 82: 414-418. [Crossref]
- Abraham Benatar, Tine Decraene, Arjen Feenstra (2010) Ruptured sinus of Valsalva aneurysm in a child with Down syndrome: a rare cardiac anomaly. Med Sci Monit 16: CS135-CS137. [Crossref]
- Wei Cui, Andrew H van Bergen, Dhaval Patel, Alex J Javois, David A Roberson (2008) Transcatheter closure of ruptured sinus of valsalva aneurysm and secundum atrial septal defect with limited inferior rim. Echocardiography 25: 208-213. [Crossref]
- Jun Ho Lee, Ji-Hyuk Yang, Pyo Won Park, Jinyoung Song, June Huh et al. (2019) Surgical Repair of a Sinus of Valsalva Aneurysm: A 22-Year Single-Center Experience. Thorac Cardiovasc Surg. [Crossref]