Rectal Cancer: Asynchronous Metastasis to the Temporal Bone, Temporomandibular Joint and Middle Ear
A B S T R A C T
Rectal cancer has the potential to metastasize to multiple anatomical sites. The hallmark of treatment presides with sound oncologic surgery, adjunct with chemotherapy and radiation therapy when indicated. The initial presentation determines the management regimen, consisting of physical examination and diagnostic imaging. A 54-year-old female presented with locally advanced rectal cancer. Upon conclusion of neoadjuvant chemotherapy and radiation therapy, she underwent a low anterior resection with total mesorectal excision. Her surgical margins were negative; however, of the 21 lymph nodes retrieved, 11 were positive for cancer. The patient underwent further adjuvant chemotherapy. 2 years, 8 months later, the patient presented to the emergency department with worsening swelling of the right side of the face, with increasing pain, hearing, and visual impairments. Diagnostic imaging revealed a large lesion in the cranial anatomy, invading the temporal bone, temporomandibular joint, sphenoid bone and anterior superior epitympanum of the right middle ear. The patient underwent operative intervention followed by radiation and chemotherapy. Asynchronous metastasis of rectal cancer to the cranium is a rare finding and an invasion into the temporal bone even more scarcely reported. The prognosis for distant metastatic disease is poor because it involves metastatic spread via the lymph channels or vascular system. Patients that have undergone treatment for advanced rectal cancer must be approached with a high index of suspicion for distant metastatic disease, even in the advent of routine negative surveillance.
Keywords
Rectal cancer, metastatic disease, asynchronous metastasis, temporal bone, sphenoid bone, temporomandibular joint, TMJ, epitympanum
Introduction
The incidence of rectal cancer in the United States was 44,180 in 2019 [1, 2]. The disease entity affects both males and females with equal distribution. Treatment regimens are based upon the staging of the disease at the time of initial presentation. Physical exam and diagnostic imaging are paramount in determining staging and the subsequent management regimen. Some important risk factors identified in developing rectal cancer include personal history of rectal cancer, rectal adenomas, family history of rectal cancer, hereditary conditions such as familial adenomatous polyposis (FAP), hereditary nonpolyposis colorectal cancer (HNPCC), inflammatory bowel disease, excessive alcohol or tobacco consumption, race and obesity, to name a few [3-12]. Classically, rectal cancer metastasizes to the liver, lungs and contiguous anatomy; however, increasingly multiple different sites have been reported, both with synchronous and asynchronous presentations.
Case Presentation
A 54-year-old female presented to her gastroenterologist with complaints of bloody bowel movements. She had noticed these over the course of the previous year but had ignored them due to their intermittent nature. Over the past month, the frequency of seeing blood increased, which prompted her to seek gastroenterology consultation. The patient’s past medical history and family history were unremarkable, but she was a smoker with a 30-pack year history. Her previous colonoscopy was more than 5 years. The patient did not describe any symptoms except for the bleeding with her bowel activities. She was well-nourished, and her physical exam was unremarkable.
The patient underwent a colonoscopy and was found to have a significant ulcerated mass in the proximal rectum. This was biopsied and proven to be adenocarcinoma. Proctoscopy was undertaken and showed the mass to be 9 cm from the anal verge. MRI and endorectal ultrasound were employed for staging and the tumor was a T3N1, based on imaging. The patient underwent baseline CEA, which was 3.7. She subsequently was referred to both medical and radiation oncology for neoadjuvant chemoradiation therapy.
Eight weeks after concluding her neoadjuvant chemoradiation treatments, the patient underwent a low anterior resection with a diverting loop ileostomy. Her pathology revealed negative proximal, distal and circumferential margins. The tumor did exhibit perineural and lymphovascular invasion. Eleven out of the 21 lymph nodes retrieved from the total mesorectal excision were positive for malignancy. The patient proceeded to adjuvant chemotherapy. 6 months after concluding her adjuvant chemotherapy, the patient’s tumor markers were normal. Her repeat imaging of the chest, consisting of PET and CT imaging of the abdomen and pelvis, were all negative. She subsequently underwent a gastrografin enema under fluoroscopy to evaluate the integrity of the colorectal anastomosis. The anastomosis was intact, and the diverting ileostomy was reversed.
2 years and 8 months later, the patient presented to the emergency room with severe pain and swelling of the right facial region. The onset of the swelling with discomfort had started 2 weeks prior; however, the patient had attributed this to ear infections and dental pain. She had sought consultation from the dentist and was prescribed antibiotics and pain medication. As her pain, vision and hearing became affected, she presented emergently to the hospital. The patient underwent a CT and MRI scan of the head in the emergency room (Figures 1 & 2).
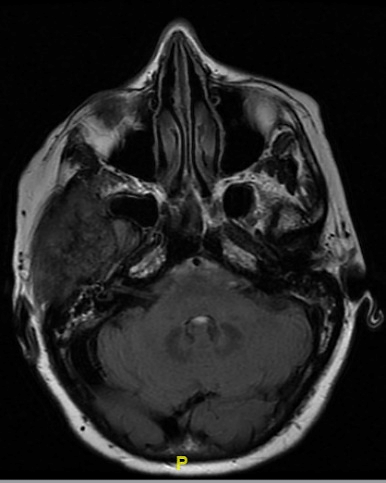
Figure 1: MRI of the head showing the tumor invading into the right temporal region.
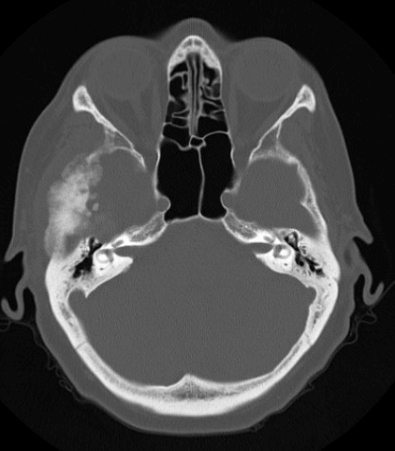
Figure 2: CT of the head showing the significant invasion into the temporal bone structure.
The findings were profound. The patient had interval development of fibro-osseous tumor in the right temporal squamous portion involving the floor of the right middle cranial fossae and right articular fossa of the temporomandibular joint. The central osteogenic component of the tumor was surrounded with a rim of soft tissue component, lytic changes of the right sphenoid bone, with extension and involvement of the anterior superior epitympanum of the right middle ear. An immediate consultation was obtained from neurosurgery, otolaryngology and oral and maxillofacial surgery services.
The patient was taken to the operating room where she underwent right temporal craniectomy, complex debulking of the tumor with facial reconstruction and closure. The pathology of the facial mass was metastatic colorectal adenocarcinoma with mucinous features. The pathology was compared with the original rectal cancer, and it was determined that the origin of the new asynchronous location was indeed the rectal cancer from almost 3 years ago.
Following recovery from surgery, the patient was restarted on chemotherapy and received adjuvant radiation. She successfully completed her radiation, continues to be on chemotherapy but is doing well.
Discussion
Rectal cancer metastasis to the temporal bone is an uncommon finding. Metastasis, in general to the temporal bone, is rare, with previously reported large studies in the literature only able to compile 134 cases [13]. The majority origin of the de novo cancers were, in decreasing order, breast, lung, kidney, prostate and stomach [14]. Other isolated case reports of metastatic disease into the temporal bone included synchronous findings of a colon cancer primary [15]. Asynchronous findings were exceedingly rare in the literature [15].
Data from the Swedish cancer registry, 49,096 patients, found rectal cancer to metastasize most commonly into the solid organs (the most common being the liver) and the thoracic cavity. The nervous system and peritoneum were less common, with the exception of cancers with a mucinous component. The mucinous subtype did spread into the peritoneum with increased frequency [16]. There have been many theories explaining the distant metastatic spread of rectal cancer. Lymphatic channels offer both portal and systemic spread. Tumor spread involving veins is thought to offer ease of distant metastasis, avoiding further tumor detection with access to anatomy reliant upon vasculature [17].
Our patient presented with symptoms 2 years and 8 months following her original diagnosis of rectal cancer. While her treatment was well tolerated and she was deemed to be in remission, the cancer did return to a remote site. Her surveillance colonoscopies and imaging of the abdominal and pelvic cavity had all been negative. Her tumor markers continued to be within the normal parameters. There have been studies documenting the most favourable prognosis of metastatic rectal cancer to be in patients with isolated lung metastasis; however, the overall prognosis of metastatic rectal cancer is poor [18]. We recommend that every patient with a history of rectal cancer, in particular those within 5 years of treatment, undergo a thorough metastatic workup should they present with clinical signs and symptoms not readily explained. As the century-old medical nomenclature reads, cancer does not follow rules or read a textbook! The clinician’s index of suspicion must remain high to combat the truly terrible disease.
Article Info
Article Type
Case ReportPublication history
Received: Wed 08, Apr 2020Accepted: Thu 23, Apr 2020
Published: Mon 27, Apr 2020
Copyright
© 2023 Ali Mahmood. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.04.08
Figures & Tables
References
- National Cancer Institute (2019) Rectal Cancer Treatment (PDQ®)–Health Professional Version.
- American Cancer Society (2019) Cancer Facts and Figures. Atlanta, GA.
- Johns LE, Houlston RS (2001) A systematic review and meta-analysis of familial colorectal cancer risk. Am J Gastroenterol 96: 2992-3003. [Crossref]
- Imperiale TF, Juluri R, Sherer EA, Glowinski EA, Johnson CS et al. (2014) A risk index for advanced neoplasia on the second surveillance colonoscopy in patients with previous adenomatous polyps. Gastrointest Endosc 80: 471-478. [Crossref]
- Singh H, Nugent Z, Demers A, Czaykowski PM, Mahmud SM et al. (2013) Risk of colorectal cancer after diagnosis of endometrial cancer: a population-based study. J Clin Oncol 31: 2010-2015. [Crossref]
- Srinivasan R, Yang YX, Rubin SC, Morgan MA, Lewis JD (2007) Risk of colorectal cancer in women with a prior diagnosis of gynecologic malignancy. J Clin Gastroenterol 41: 291-296. [Crossref]
- Mork ME, You YN, Ying J, Bannon SA, Lynch PM et al. (2015) High Prevalence of Hereditary Cancer Syndromes in Adolescents and Young Adults with Colorectal Cancer. J Clin Oncol 33: 3544-3549. [Crossref]
- Laukoetter MG, Mennigen R, Hannig CM, Osada N, Rijcken E et al. (2011) Intestinal cancer risk in Crohn's disease: a meta-analysis. J Gastrointest Surg 15: 576-583. [Crossref]
- Fedirko V, Tramacere I, Bagnardi V, Rota M, Scotti L et al. (2011) Alcohol drinking and colorectal cancer risk: an overall and dose-response meta-analysis of published studies. Ann Oncol 22: 1958-1972. [Crossref]
- Liang PS, Chen TY, Giovannucci E (2009) Cigarette smoking and colorectal cancer incidence and mortality: systematic review and meta-analysis. Int J Cancer 124: 2406-2415. [Crossref]
- Laiyemo AO, Doubeni C, Pinsky PF, Doria Rose VP, Bresalier R et al. (2010) Race and colorectal cancer disparities: health-care utilization vs different cancer susceptibilities. J Natl Cancer Inst 10: 538-546. [Crossref]
- Lansdorp Vogelaar I, Kuntz KM, Knudsen AB, van Ballegooijen M, Zauber AG et al. (2012) Contribution of screening and survival differences to racial disparities in colorectal cancer rates. Cancer Epidemiol Biomarkers Prev 21: 728-736. [Crossref]
- Kobayashi K, Igarashi M, Ohashi K, McBride R (1986) Metastatic seminoma of the temporal bone. Arch Otolaryngol Head Neck Surg 112: 102-105. [Crossref]
- Ruah CB, Bohigian RK, Vincent ME, Vaughan CW (1987) Metastatic sigmoid colon adenocarcinoma to the temporal bone. Otolaryngol Head and Neck Surg 97: 500-503. [Crossref]
- MacAfee KA 2nd, Quinn PD, Abaza NA (1993) Adenocarcinoma of the Colon Metastatic to the Temporomandibular Joint: A case report. Journal of Oral and Maxillofacial Surgery. J Oral Maxillofac Surg 51: 793-797. [Crossref]
- Samlali H, Bouchbika Z, Bennani Z, Taleb A, Benchekroune N et al. (2017) Brain metastasis from rectal adenocarcinoma: about a case and review of the literature. Pan Afr Med J 26: 58. [Crossref]
- Riihimäki M, Hemminki A, Sundquist J, Hemminki K (2016) Patterns of metastasis in colon and rectal cancer. Sci Rep 6: 29765. [Crossref]
- Lord AC, Knijn N, Brown G, Nagtegaal ID (2020) Pathways of spread in rectal cancer: a reappraisal of the true routes to distant metastatic disease. Eur J Cancer 128: 1-6. [Crossref]
- Prasanna T, Karapetis CS, Roder D, Tie J, Padbury R et al. (2018) The survival outcome of patients with metastatic colorectal cancer based on the site of metastases and the impact of molecular markers and site of primary cancer on metastatic pattern. Acta Oncol 57: 1438-1444. [Crossref]