Novel Chest Tube Anchoring and Closure Technique with an Aesthetic Scar
A B S T R A C T
Technique: This chest tube anchoring technique differs from other techniques by introducing 2 layered closure to avoid wound healing complications such as hypertrophic or keloid scar and to achieve airtight closure. The first suture to be used is a monofilament synthetic absorbable 4/0 suture – Monocryl (Johnson & Johnson, New Jersey, USA) that is passed as a buried stitch in the dermal layer. The second suture to be used is a monofilament non-absorbable 3/0 suture – Prolene (Johnson & Johnson, New Jersey, USA) that is passed around the chest tube incision in a horizontal mattress manner taking the muscle/fascia and skin layers. The chest tube is then anchored with a 2/0 silk suture with a mesentery. The three suture ends are secured and wrapped around the chest tube with Steri-Strips™ (3M™, Minnesota, USA). Two long dressings are sandwiched together, partially on skin and partially on the tube as dressing anchors.
Results: This technique has shown good results with no complications. Routine chest radiograph and physical examination showed no signs of pneumothorax or discharge from the wound nor any wound healing complications.
Conclusion: This chest tube anchoring and closure technique is secure and produces an aesthetic pleasing scar that does not require any expensive sutures or special skills.
Keywords
Chest tube anchor technique, chest tube closure technique, aesthetic chest tube scar
Introduction
Chest drains are indicated in different clinical situations such as after thoracic surgeries or in patients who sustained pneumothorax or haemothorax. The primary aim of drain anchorage is to avoid dislodgement and many techniques have been described [1-4]. It usually involves using a single ‘mattress’ suture that purse strings the wound together. This method often gives undesirable result as the linear wound is converted into a circular one that leaves an unsightly scar or keloid formation [1, 2]. Two methods have been proposed to improve the chest tube scar by using barbed knotless suture and no suturing technique [4-6]. Improvement in scar cosmesis is seen but they both reported low incidence of pneumothorax and serous discharge after drain removal that required intervention [5, 6].
In our institution, rib fracture fixation is performed by the plastic surgery department and chest drain is inserted for this procedure. We propose using this chest tube anchoring and closure technique that is based on our expertise on skin closure and wound care.
Technique
In the emergency setting, chest tube is inserted first then the sutures (Figure 1A). Whilst in the operating room for the latter 2 indications, the chest tube is inserted after suture placements. After local anaesthesia, a stab incision is made to accommodate the surgeon’s little finger. Dissection with artery forceps and blunt dissection with the little finger to sweep the pleura off is performed as standard practice.
The first suture placed is the monofilament 4/0 suture-Monocryl (Johnson & Johnson, New Jersey, USA) that is passed as a buried stitch in the dermal layer (Figure 1B). This monocryl suture serves as the foundation for optimal wound healing and scar formation as it reduces the tension on the epithelium and everts the skin edges. A second suture using a monofilament 3/0 suture – Prolene (Johnson & Johnson, New Jersey, USA) is passed around the chest tube incision in a horizontal mattress taking the muscle/fascia and skin layers (Figure 1C). This Prolene suture ensures airtight closure by including the muscle/fascia and skin layers; and it causes minimal skin reactivity avoiding complications such as hyperpigmentation. Once the two sutures for closure are in place, the chest tube is anchored with a 2/0 silk suture with a mesentery to allow mobility of the drain to prevent tension and kinking (Figure 1D). The mesentery also prevents undue pressure points on the skin which causes inflammation and erythema that can contribute to hyperpigmentation, poor scarring and pain. The ends of the 3 sutures are secured and wrapped individually with Steri-Strips™ (3M™, Minnesota, USA) around the chest tube. Two long dressings are sandwiched together longitudinally so that it sits partially on skin and tube as dressing anchors. We have stopped the need for pressure taping and its complications such as skin blistering and restriction of chest moment during respiration [2].
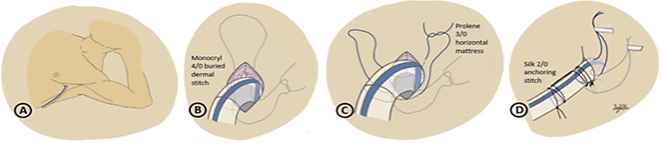
Figure 1: A-D) Chest tube anchoring technique.
Once the chest tube is due for removal, the ends of the sutures are unwrapped from the chest tube (Figure 2A). The sutures are easily identified as they have different colours – prolene is blue, monocryl is clear and silk is black. Clear identification of the sutures can minimise the mistake of taking out the wrong suture. The assistant withdraws the chest tube while the patient is at full inspiration. First, the prolene stitch is hand tied to seal the wound once the chest tube is removed (Figure 2B). Subsequently, the monocryl suture is hand tied to close the underlying dermal layer (Figure 2C). Steri-Strips™ (3M™, Minnesota, USA) are applied to the wound to oppose the epithelium layer and further reduce tension to avoid poor scarring. The prolene stitch on the skin is removed after 4-5 days to avoid suture tracks scarring.
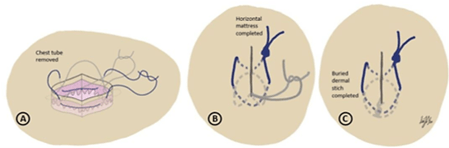
Figure 2: A-C) Post chest tube removal closure technique.
Routine chest radiograph and physical examination showed no signs of pneumothorax or wound discharge. There has been no wound dehiscence, wound infection or painful scar observed (Figure 3).
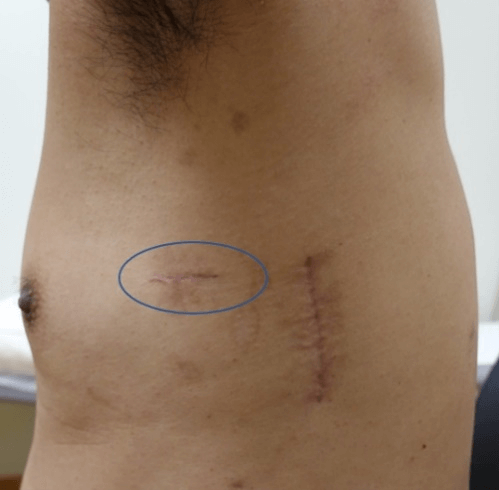
Figure 3: Chest tube scar (circled).
Discussion
Many chest tube anchoring techniques have been described but not many focus on wound healing and scar formation. Hypertrophic or keloid scars often cause pain and itchiness that can be morbid to patients and require long term medical treatment. This technique improves on the traditional method by introducing a 2 layered closure. Benefit of having 2 sutures is that the dermal stitch distributes tension between the dermal layer and the muscle/fascia layer as opposed to single composite closure. It also serves to evert wound edges to avoid poor scarring. The preservation of the ‘standard’ monofilament prolene suture allows for airtight closure. This suture also serves to prevent muscle separation which can lead to poor and depressed scarring. This suture also minimises dead space reducing the risk of seroma formation resulting in wound discharge.
Our method does not require any expensive suture such as barbed suture that incurs extra cost [4]. In addition, barbed dermal suture only provides dermal-epidermal closure of the wound thus not guarantee airtight closure and increases risks of muscle separation leading to depressed or poor scarring. The method we propose does not require any adjustment to the incision in order to pass the needle through that might be required in the barbed suture technique [4]. The method by Rashid involves placing 2 sutures at the ends of the wound to oppose the two ends primarily and then a central horizontal mattress suture for skin closure [1]. This method is unnecessary in our technique as there is a dermal continuous stitch to oppose the entire wound. So far, no chest tube anchoring techniques have been proven to be ideal. This chest tube anchoring and closure technique is secure and produces an aesthetic pleasing scar that does not require any expensive sutures or special skills.
Acknowledgment
Lim Jia Xu, National Neuroscience Institute, Singapore.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Short CommunicationPublication history
Received: Mon 21, Dec 2020Accepted: Mon 04, Jan 2021
Published: Mon 18, Jan 2021
Copyright
© 2023 Vigneswaran Nallathamby. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.01.08
Figures & Tables
References
- Rashid MA, Wikström T, Ortenwall P (1998) A simple technique for anchoring chest tubes. Eur Respir J 12: 958-959. [Crossref]
- Laws D, Neville F, Duffy J (2003) BTS guidelines for the insertion of a chest drain. Thorax 58: ii53-ii59. [Crossref]
- Kim MS, Cho JH (2017) A new method of chest drain wound closure using knotless suture material. Ann Thorac Surg 103: e93-e95. [Crossref]
- Kim KS (2017) Barbed suture material technique for wound closure and concomitant tube placement in uniportal VATS for pneumothorax. J Thorac Dis 9: 1265-1272. [Crossref]
- Smelt JLC, Simon N, Veres L, Harrison Phipps K, Bille A (2018) The Requirement of Sutures to Close Intercostal Drains Site Wounds in Thoracic Surgery. Ann Thorac Surg105: 438-440. [Crossref]
- Kim MS, Shin S, Kim HK, Choi YS, Kim J et al. (2018) Feasibility and Safety of a New Chest Drain Wound Closure Method with Knotless Sutures. Korean J Thorac Cardiovasc Surg 51: 260-265. [Crossref]