Non-Invasive Treatment of Adolescent Idiopathic Scoliosis: Systematic Literature Review by Using Citation Network Analysis
A B S T R A C T
There are many nonsurgical treatment options from adolescent idiopathic scoliosis (AIS) to control the progression of the spinal curvature. However, the existing studies are so diverse and diffuse that it is challenging to find potential trends for further studies without a more comprehensive review in place for reference purposes. Thus, the objective of this review article is to conduct a systematic literature review on the noninvasive treatment of AIS with a citation network analysis. The Web of Science (WoS) was searched using 9 reference keywords to collect published articles in English on nonsurgical treatment options for AIS from 1979 to 2019. Each eligible article focused on the nonsurgical options for treating AIS. In addition, the HistCite and the UCINet softwares were referred to for article distribution and citation network analysis. Only non-invasive treatment options of AIS were included. Studies that estimated the amount of spinal curvature, causes of or risk factors for AIS and any invasive treatments, such as surgery, were not focused on. The articles were independently extracted by 3 authors based on the predefined eligibility criteria. The title, authors, year of publication, country or region of publication, reference list, keywords and other bibliographic information from each article was extracted and analyzed purely based on the data with the HistCite and UCINet programs. At last, a total of 146 articles out of 1594 articles were selected for the literature review after the exclusion of 1357 irrelevant articles and 91 inappropriate studies, such as letters and proceedings papers. Of these 146 articles, the majority were empirical studies (74.0%). There was also a lack of meta-analyses in this research field. Based on the results of the citation network analysis, most of the top 10 articles with the highest local citation scores (LCSs) focused on bracing as a treatment. The popularity of bracing as a research topic was also supported by the citation network structure, as brace treatment was in the largest of the five research clusters; this cluster also included posture training through exercise, managing the corrective forces of braces, 3D analysis of braces and quality of life during brace treatment. However, most of these studies focused on rigid braces. A few studies on non-rigid braces and other types of nonsurgical treatment were available in the current literature, which might indicate potential research areas for future studies. To conclude, noninvasive treatment for AIS has been on the academic radar recently; but there are still research gaps, such as the lack of research on semi-rigid and flexible braces or posture training exercises with biofeedback systems. Further studies could explore these research directions.
Keywords
Adolescent idiopathic scoliosis, noninvasive treatment, spinal curvature, brace treatment, exercise, observation, citation network analysis
Introduction
Adolescent idiopathic scoliosis (AIS) is the most common pediatric spinal disorder, accounting for 80% of scoliosis cases and affecting 2-4% of children during their pubertal growth spurt, especially those between the ages of 10 and 16 years who have not yet reached skeletal maturity [1, 2]. To date, no one has concisely determined the etiopathogenesis of this three-dimensional (3D) spinal ailment. Some researchers have noted that there are three possible risk factors for spinal curvature progression: skeletal immaturity, female sex and a large curve magnitude [3, 4]. In AIS patients, a C- or S-shaped spine can be found because of trunk rotation or abnormal spinal shifts. AIS is a long-term condition in which patients can experience increased spinal curvature if appropriate treatment is not prescribed [1, 5]. AIS not only can lead to many problems, such as posture issues and cosmetic defects, but it can also cause health issues such as back pain and cardiopulmonary diseases, which are likely to affect the quality of life of patients [6]. Thus, monitoring and controlling spinal curvature is a priority for all AIS patients.
To minimize the progression of the spinal curvature, different treatment options are prescribed for patients based on the Cobb angle severity. Generally, observation, brace treatment and surgery are the three main current types of treatment recommended for AIS [7, 8]. For mild cases (spinal curvature angles of 10-20 degrees), observation is always the main type of prescribed treatment. Sometimes, exercises or physiotherapy are also suggested. For moderate cases with Cobb angles between 21 and 40 degrees, bracing is preferred. Although semi-rigid and flexible braces can also influence the development of the spine, rigid braces are the most common types of braces used [9-13]. Regardless of the type of brace that patients choose, they must commit to wearing the brace for a few years, until they reach skeletal maturity. For patients with more severe scoliosis and a spinal curvature of over 45 degrees, surgery is usually recommended.
To minimize the need for surgery, nonsurgical treatment options are given careful consideration. Examples of such treatments include physiotherapy, Schroth's exercises and scoliosis-specific exercises, treatment with the Boston and Ch�neau braces and the C-brace, chiropractic sessions, lateral electrical surface stimulation, and so on. Most of the outcomes of such treatment are diverse and diffuse. The variability of nonsurgical treatment, the lack of consensus on bracing options and the uncertainties regarding certain exercises are all challenges of selecting the most appropriate option for treating AIS. To investigate the current studies in this research field and determine potential areas for future research, comprehensive and systematic reviews are required. In general, a systematic literature review (SLR) can help to classify a dataset into different research domains and represent different knowledge structures. However, both the research domain and the knowledge structure are commonly identified and determined by the author, which are the limitations of an SLR [14, 15].
A citation network analysis (CNA), which is a new collection of tools used to determine the dynamics of a field via a computer-based systematic analysis of its bibliographic data, is introduced into an SLR to avoid the subjective bias of the author [14]. After all, researchers are likely to cite one another and recommend or examine a new phenomenon that modifies a previous contribution in the same research field. In other words, the development and improvement of knowledge in the field can thus be enhanced by a CNA. According to Hummon and Dereian, not only would the use of a CNA help to prevent the prevalence of formless sets of articles that are based on citations, but it would also generate a system of channels that transform scientific knowledge based on previous work in the field [16]. Therefore, a CNA can offer the potential to ensure high-quality results, classify research clusters more successfully and is more objective than the traditional SLR [14, 15]. However, there are few comprehensive and systematic reviews of these alternative types of AIS treatments, and no literature review in this area has used CNA.
This review article will thus present a systematic analysis of relevant studies. The objectives of this study are as follows: 1) to summarize previous studies on noninvasive treatment for AIS, 2) to determine and map the major research clusters of noninvasive treatment based on a CNA of the examined articles, and 3) to summarize the general trends and provide potential areas for future research.
Methods
This study followed the research methodology of Colicchia and Strozzi and Wetzstein et al. (Figure 1) [14, 17].
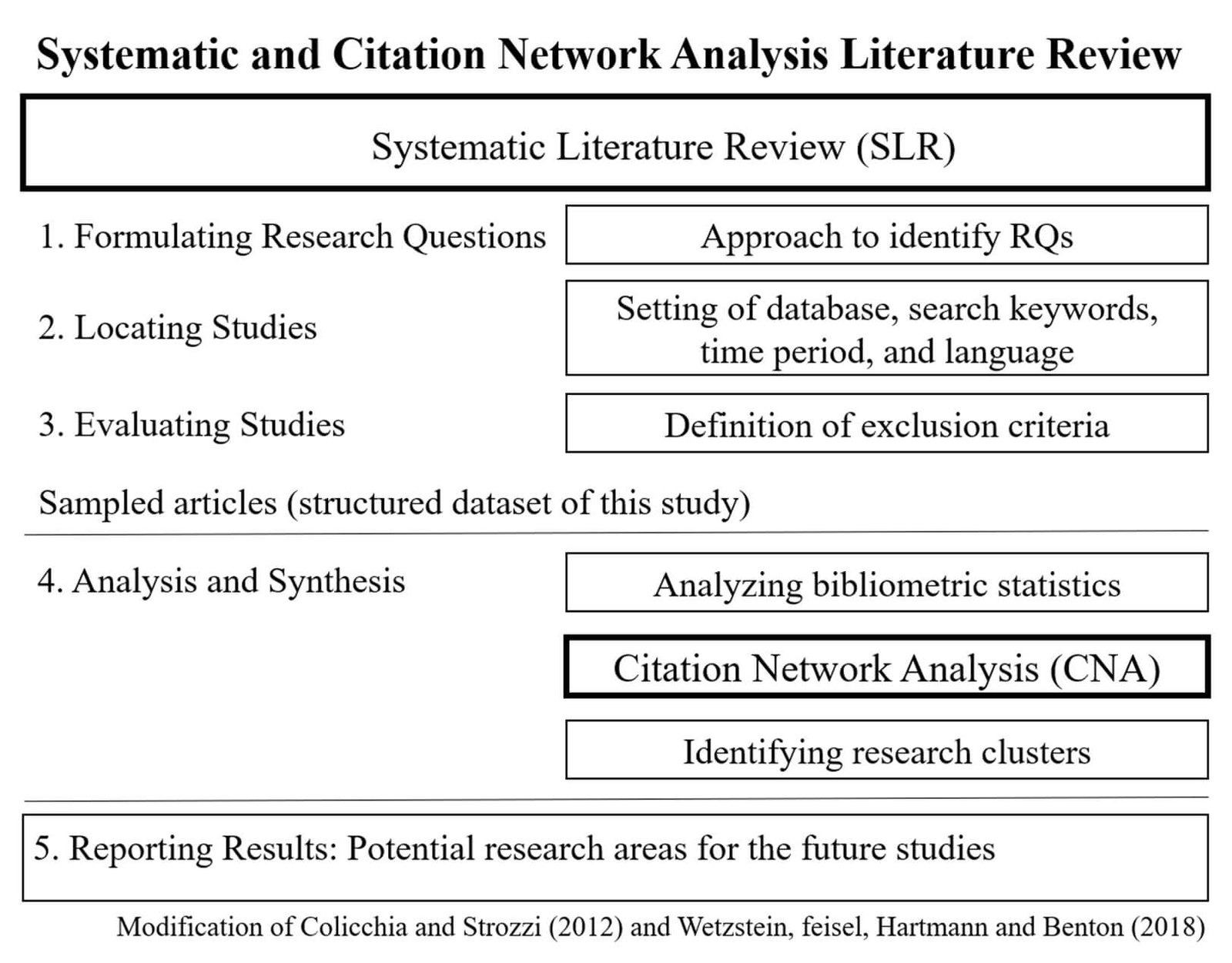
Figure 1: Research Methodology (modification [14, 17]).
For this objective literature review with a computer-based systematic analysis, a full-text search of journal articles was carried out using the Web of Science (WoS) database to collect the sample articles. Based on the most common keywords used in existing reviews and relevant research studies, the terms "adolescent idiopathic scoliosis", "curvature deformation", "spinal curvature", "Cobb's angle", "exercise", "brace treatment", "quality of life", "conservative treatment" and "nonoperative treatment" were selected and inputted as the reference keywords. To reduce the possibility of overlooking articles, similar phrases and specific types of treatments, such as "Boston brace" and "Schroth's exercises", were also included. More importantly, as only nonsurgical treatments for AIS were considered in the literature review, it was necessary to ensure that all surgical procedures were excluded in the search, which was conducted as outlined below.
Inclusion terms: "TS=(adolescent idiopathic scoliosis) AND TS=(conservative treatment OR conservative approaches OR curvature deformation OR curvature deformity OR spinal deformation OR spinal deformity OR progression OR curve progression OR spinal decompensation OR angle OR Cobb's angle OR large curves OR spinal curvature OR efficacy OR quality OR quality-of-life OR reduce OR impact OR system OR program OR therapy OR trial OR guideline OR monitoring OR exercise OR exercises OR evidence-based practice OR scoliosis-specific exercises OR stabilization exercise OR general exercise OR physiotherapy OR Schroth OR rehabilitation OR postural rehabilitation OR active training OR active-self-correction OR postural training OR SEAS.02 exercises OR exercise movement techniques OR spinal manipulation OR brace OR braces OR bracing OR brace treatment OR Chenean brace OR Boston brace OR Boston OR Wilmington brace OR Spinecor OR Charleston bending brace OR Milwaukee brace OR non-invasive treatment OR non-operative treatment OR non-operative management OR noninvasive treatment OR nonoperative treatment OR nonoperative management)". Exclusion terms: "NOT TS=(surgery OR surgeries OR surgical OR operation OR operative OR operative treatment OR invasive treatment OR off-brace OR after brace treatment OR after bracing treatment OR after wearing hard brace OR after wearing brace OR prediction)"
Since the WoS database started to collect related articles in 1979, all of the target articles about non-operative treatments of AIS patients of any age and gender that included the relevant keywords were written in English and were published between 1979 and 2019. The last search was run on 12 February 2019. Furthermore, no specific countries, regions or type of study designs were included or excluded during the search process. The research trend, types of treatments, clusters, and the quantities of related studies and citation of all included articles were focused as outcome measures in this study. The 3 authors of this study selected the relevant papers from the collected articles independently based on the predefined eligibility criteria to ensure that all the selected articles were relevant and related to the non-operative treatments of AIS and minimize the opportunities of missing articles and personal bias. Consensus was reached when there were disagreements between authors during article selection.
To apply the CNA approach in this review article, citation and reference data were collected using the WoS database and analyzed with the HistCite and UCINet programs. Upon completion of the article retrieval process, a number was assigned to each article. The title, authors, year of publication, country or region of publication, reference list, keywords and other bibliographic information from each article were documented in a citation matrix. The citation matrix was then imported into HistCite, a software program used for bibliometric analysis and information visualization [18]. This matrix showed the article distribution based on the name of the journal, publication year, country of author, type of article and method used and could be used to identify the most frequently cited papers on nonsurgical treatment for AIS. Such representations are considered a type of CNA with basic suppositions related to the extent of citation. Pilkington and Meredith stated that influential articles should be cited multiple times by other scholars, which indicates the importance and influence of their work in the field relative to articles with fewer citations [19]. The number of times that a study is cited can be determined by using two main citation scores: the local citation score (LCS) and the global citation score (GCS). The former represents the number of citations by other papers within a specific database, whereas the latter represents the number of citations by other papers worldwide. These citation scores were used to classify the relatively more noteworthy relevant articles in this database.
In addition, UCINet 6, another software program recommended by Borgatti, Everett and Freeman that can be used to analyze citation network data, was also used for information visualization to obtain a better visual result [20]. A Girvan-Newman algorithm of this software, which is a clustering algorithm designed to identify the common structure in complex systems, was applied to further examine the knowledge structure of this research area [21, 22]. This hierarchical method examines the main clusters by asking, "what is the edge that connects the largest number of articles?" Then, the irrelevant edge is removed. This process is dubbed "edge-betweenness" (EB) by Girvan and Newman and indicates the number of shortest paths between a pair of nodes [22]. Nodes with high EB are considered the highly central nodes in the network. They are then classified and separated from one another by the number of paths that pass over an edge, which allows research clusters to be identified [22].
To avoid bias and obtain a higher clustering value, the betweenness of all the edges affected by edge removal was recalculated. The quality and reliability can be evaluated through the Q-value proposed by Newman and Girvan, which was also taken into consideration in this review during cluster classification [23]. After obtaining the descriptive statistics and main research clusters from citation network structure, further analysis like article distribution in terms of type of treatment or other aspects was carried out manually.
Results
I Study Selection and Data Extraction
A total of 237 relevant articles were selected by the 3 authors of this study after scanning the titles and abstracts and then removing all irrelevant papers, such as those pertaining to genetic factors of AIS, strokes, predictions of curve progression, causes or risk factors of AIS, and any invasive treatments, such as surgery. To ensure that only articles were included, all proceedings papers, letters, editorial materials, reviews and editorial abstracts identified through HistCite were also excluded. Because review articles always review some or all non-invasive treatment options for AIS simultaneously, they are difficult to distribute and categorize into certain research clusters with CNA; consequently, all reviews shown in HistCite were removed from the database. Proceedings papers and meeting abstracts were also excluded from the database due to insufficient evidence supporting these studies. Finally, 146 out of 1594 articles were selected as the sample for this literature review. A detailed flow diagram is shown in (Figure 2). The citation matrix of selected articles was then imported into HistCite and UCINet software for the automatic data extraction and analysis.
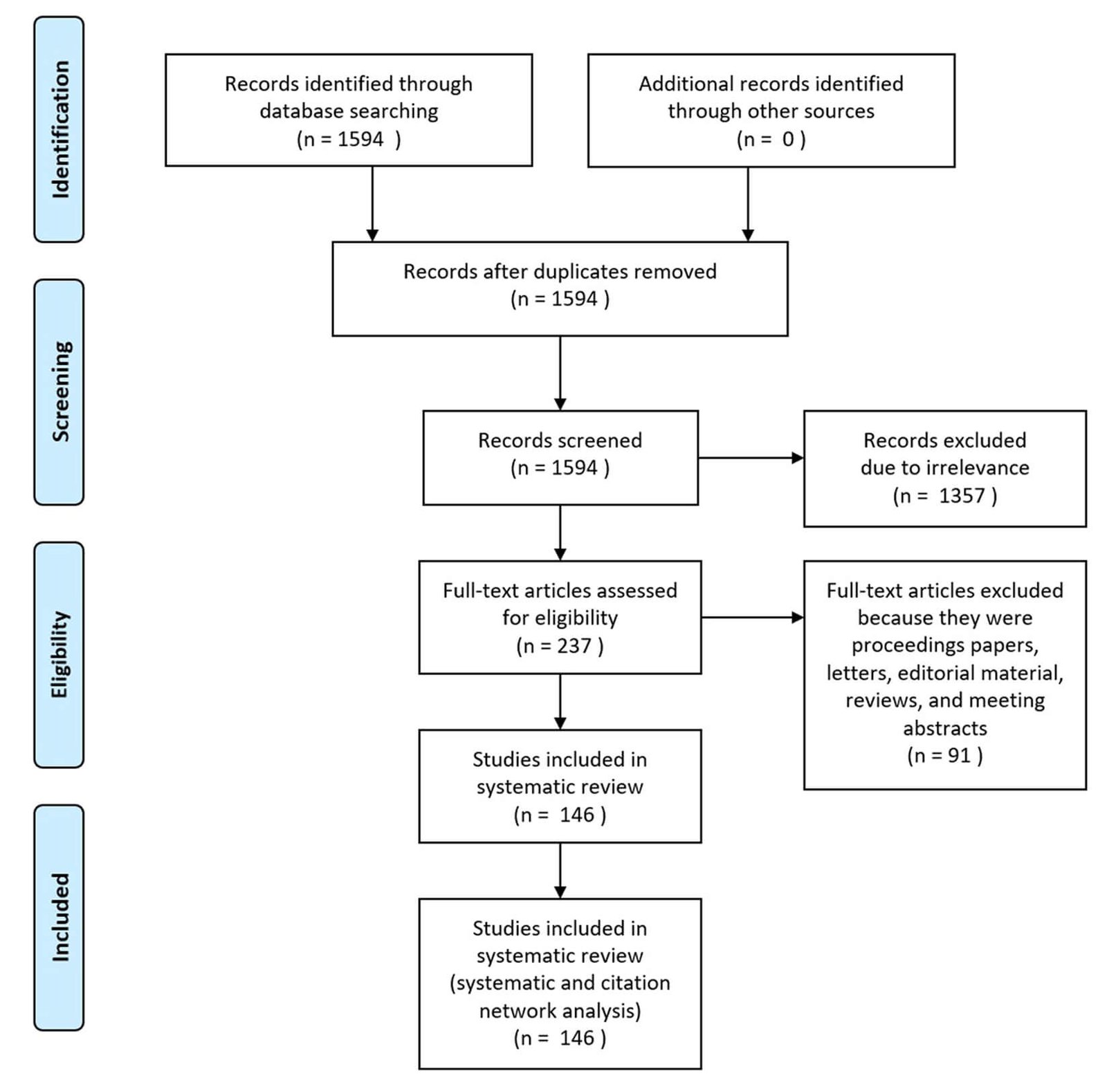
Figure 2: Flow diagram of the method.
II Descriptive Statistics
HistCite was used to distribute all 146 selected articles according to publication year, journal name, and type of article. There were no relevant papers for 2019 at the time of the study, so (Figure 3) shows the yearly output from 1979 to 2018 (and not 2019). Regarding trends in the type of articles published during this time period, it appears that researchers have become increasingly more interested in nonsurgical treatment options for AIS over time. Many such papers (32.9%) have been published in the last four years (that is, between 2015 and 2018).
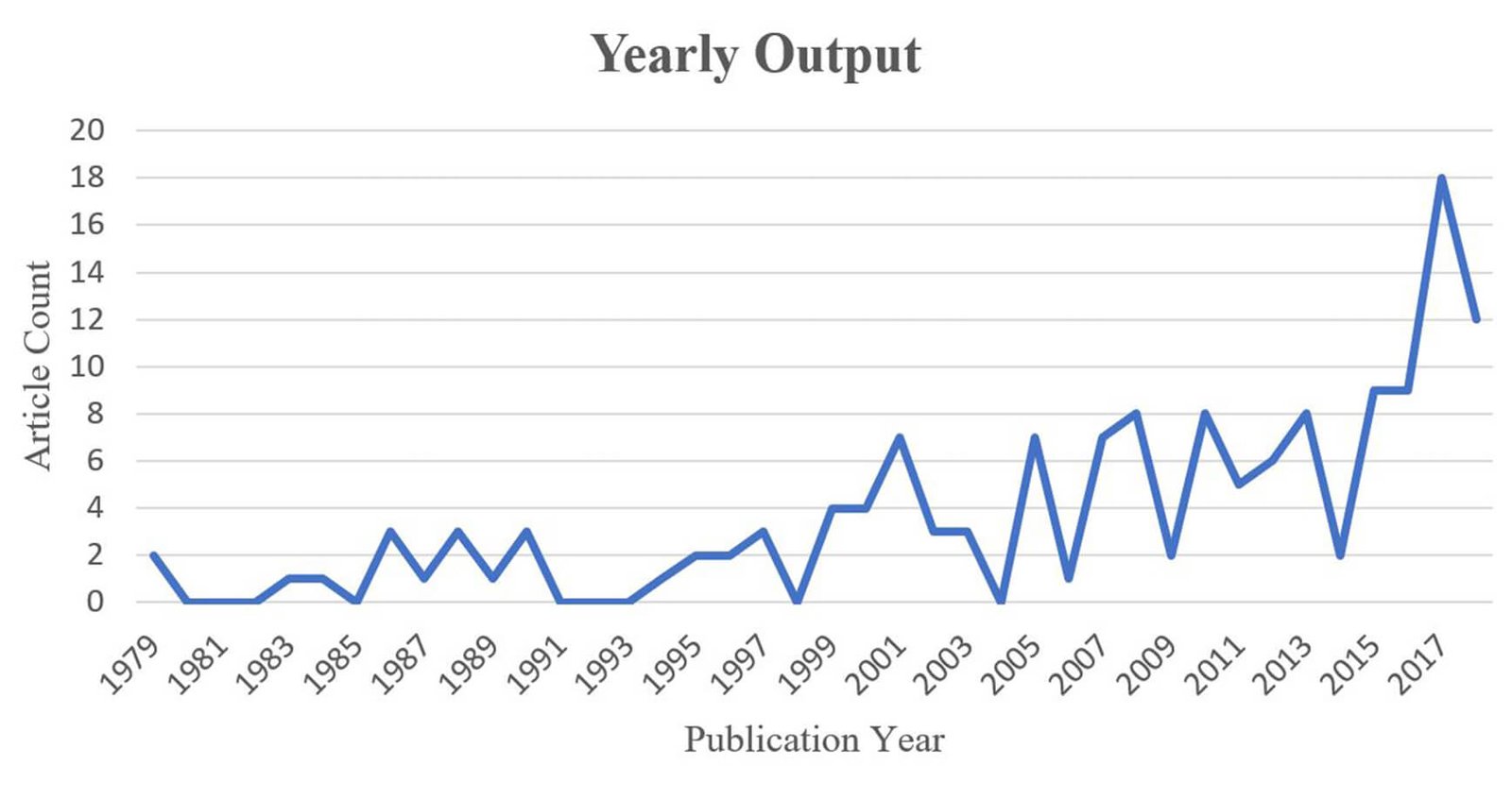
Figure 3: Article distribution in terms of yearly output.
Moreover, the 146 articles were published in 67 journals, and 10 journals published over half of the articles (52.1%), see (Figure 4). This distribution shows that these 10 journals are likely more interested in research on noninvasive types of AIS treatment; Spine, in particular, published the largest number of related papers in the sample (13%). Spine could thus be considered the most popular journal for publications in this research area.
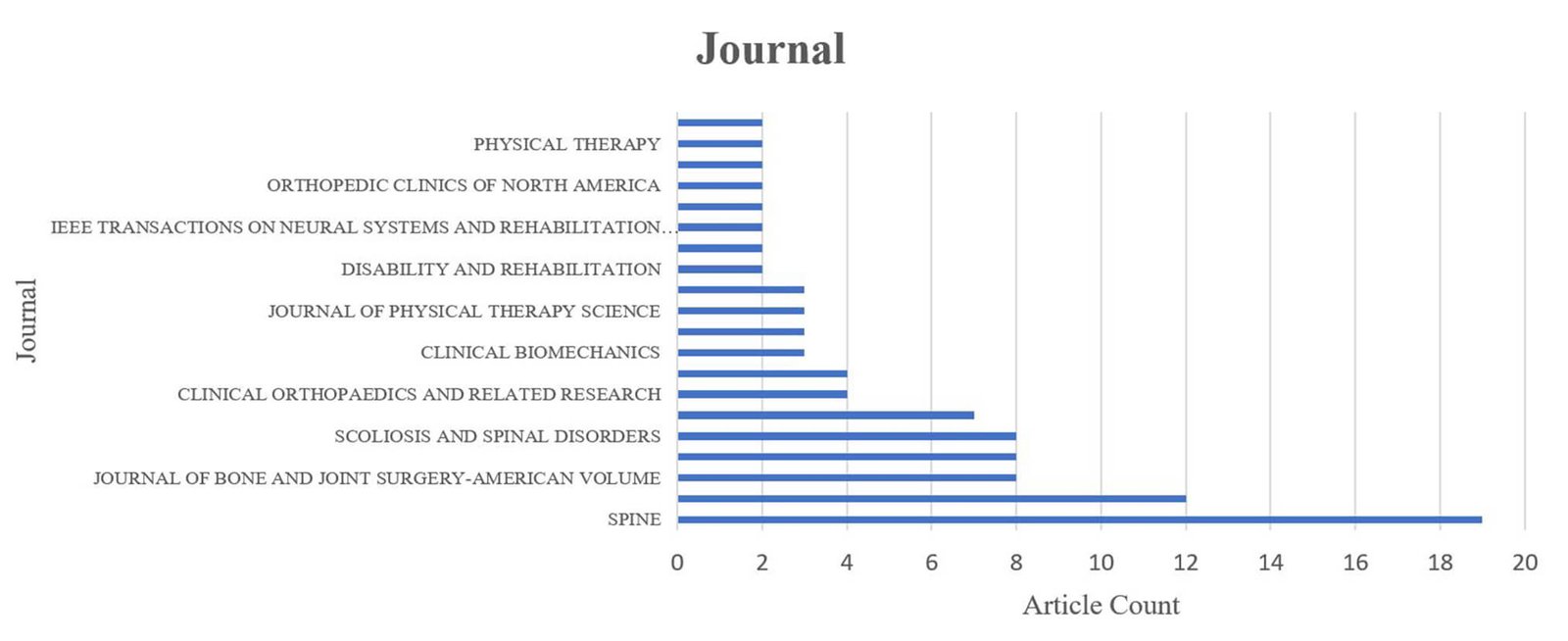
Figure 4: Article distribution based on journal.
Regarding the type of article in this database, (Figure 5) shows that most of the eligible articles were empirical research, which accounted for 108 (74.0%) of the 146 articles, while the remainder were mainly review studies (9.6%), modeling studies (8.9%), and conceptual research (6.8%). Only one meta-analysis article was found among the included articles; it was conducted by Rowe et al. [24]. This shows that nonsurgical options for treating AIS have not been studied using meta-analyses, suggesting that this might be a potential research area for future studies.
In addition, the 146 shortlisted studies originated from authors in 32 different countries. The five countries with the most shortlisted publications are shown in (Table 1). Academics in the United States of America (USA) have published the most articles on nonsurgical treatment of AIS, with 35 articles or 24% of the total number of shortlisted publications; the USA is followed by Canada, with 25 articles (17.1%); China, with 17 articles (11.6%); and two countries with relatively fewer articles: Italy, with 8 articles (5.5%), and France, with 7 articles (4.8%).
Regarding the type of article in this database, (Figure 5) shows that most of the eligible articles were empirical research, which accounted for 108 (74.0%) of the 146 articles, while the remainder were mainly review studies (9.6%), modeling studies (8.9%), and conceptual research (6.8%). Only one meta-analysis article was found among the included articles; it was conducted by Rowe et al. [24]. This shows that nonsurgical options for treating AIS have not been studied using meta-analyses, suggesting that this might be a potential research area for future studies.
In addition, the 146 shortlisted studies originated from authors in 32 different countries. The five countries with the most shortlisted publications are shown in (Table 1). Academics in the United States of America (USA) have published the most articles on nonsurgical treatment of AIS, with 35 articles or 24% of the total number of shortlisted publications; the USA is followed by Canada, with 25 articles (17.1%); China, with 17 articles (11.6%); and two countries with relatively fewer articles: Italy, with 8 articles (5.5%), and France, with 7 articles (4.8%).
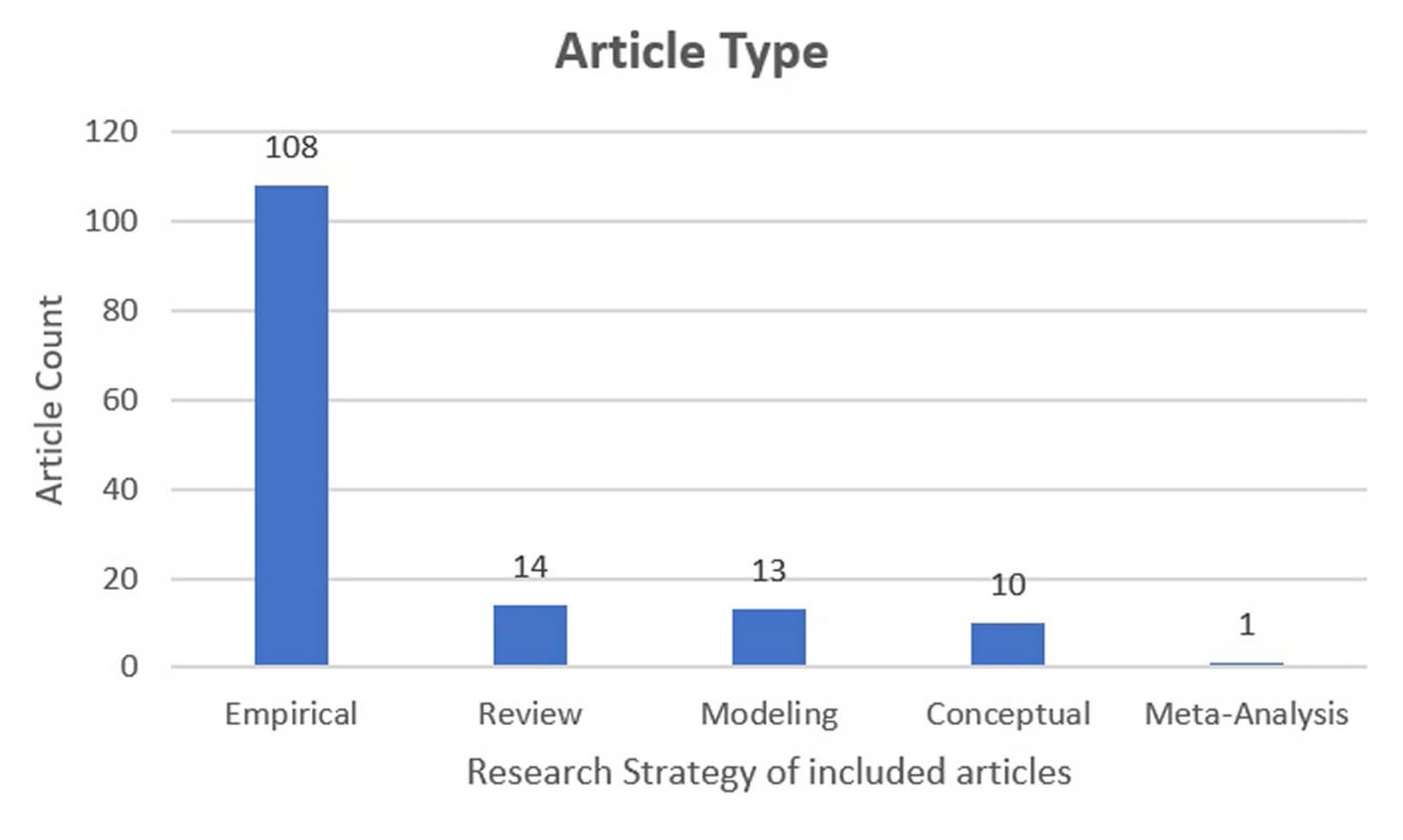
Figure 5: Article distribution based on the type of article.
Table 1: Article distribution: top 5 countries.
|
Country |
Number of included articles |
|
USA |
35 |
|
Canada |
25 |
|
China |
17 |
|
Italy |
8 |
|
France |
7 |
In addition to the article distribution presented above, HistCite was also utilized to identify the most dominant papers on noninvasive treatment for AIS. For the purposes of this review, the LCS was a much more useful and relevant score because it would focus on the 146 articles in the sample, which approximates the research field of interest. The top 10 articles with the highest LCS are listed and ranked in (Table 2) [24-33]. The papers with the highest LCS were all closely related; in particular, Nachemson et al. had the highest LCS and could be considered the most noteworthy article in this database [31].
III Identifying Research Clusters
While the statistics above show the LCS and the distribution of papers based on different factors, the knowledge structure is also important; therefore, it was elucidated using UCINet 6 software. Generally, a higher Q-value means better classification [23]. However, not all Q-values estimated by software are acceptable. Following Newman and Girvan, the optimal citation network is obtained only when the highest Q-values, those that fall within a normal range of 0.3 to 0.7, are attained [23].
In this review, the Q-value was also determined during Girvan-Newman clustering (Figure 6). The highest value was 0.376 when the algorithm divided all the included articles into 23 clusters, which is potentially the best method. Among these 23 clusters, five main domains were found, whereas the remainder of the clusters were spread disorderly; they were connected to only 1 to 2 more articles, and some even had no connection with other articles. The names of each cluster were established after a review. The clusters with only 1 to 3 articles were categorized as "Other clusters" and comprised 36 articles (24.7%) in total. As shown in (Figure 7), the largest research cluster was brace treatment, which accounted for 56 articles (38.4%), followed by posture training through exercise, with 29 articles (19.9%); 3D analysis of braces, with 11 articles (7.5%), and two other relatively smaller clusters that included studies on corrective force management and quality of life with brace treatment, and comprised a total of 7 articles (4.8%) each. The citation network structure of these six research domains, which includes the unclassified clusters (other clusters), is presented in (Figure 8).
To further investigate the specific contents studied among these two main clusters of research articles (brace treatment and posture training through exercise), the articles were differentiated by the type of brace and exercise, respectively (Figure 9). Since some of the shortlisted articles focused on more than one brace or exercise, it was difficult to identify the exact type. As a result, these articles were categorized as those with "multiple braces" or "multiple exercises". As shown in (Figure 9), the Boston brace was the most popular brace used for treatment in the brace cluster, with 20 relevant papers (35.7%), while physiotherapy was the most common form of treatment in the exercise cluster, with 5 articles on posture training through exercise (17.2%). Aside from these two main research clusters, the rest of the treatment options were rare, with only 1-3 relevant papers.
In the brace cluster, there were 24 articles studied on the effectiveness of rigid braces which were focusing on controlling the curve progression. No matter which type of rigid braces was studied in these articles, 20 of them (83.3%) agreed the spinal correction can be done effectively by wearing rigid braces, whereas other 4 articles (16.7%) doubted their corrective effect, such as the bracing effect in males, and in overweight patients with AIS [29, 34]. Although the rest of the articles in this cluster were also studying in hard braces, they focused on other aspects like modifying the fabrication of hard orthoses, as well as evaluating the static and dynamic balance control of wearers during bracing [35-38].
Table 2: Articles with the highest LCS.
|
Rank |
Author |
Title |
LCS |
|
1 |
Nachemson et al [25] |
Effectiveness of Treatment with A Brace in Girls Who Have Adolescent Idiopathic Scoliosis- A Prospective, Controlled-Study Based On Data From The Brace Study of The Scoliosis-Research-Society |
37 |
|
2 |
Emans et al [26] |
The Boston Bracing System for Idiopathic Scoliosis- Follow-up Results in 295 Patients |
27 |
|
3 |
Lonstein and Carlson [27] |
The Prediction of Curve Progression in Untreated Idiopathic Scoliosis During Growth |
19 |
|
4 |
Noonan et al [28] |
Use of The Milwaukee Brace for Progressive Idiopathic Scoliosis |
19 |
|
5 |
Rowe et al [24] |
A Meta-Analysis of The Efficacy of Non-Operative Treatments for Idiopa{Muthukrishnan, 2010 #221}thic Scoliosis |
18 |
|
6 |
Bunnell [29] |
The Natural-History of Idiopathic Scoliosis Before Skeletal Maturity |
14 |
|
7 |
Wong et al [30] |
Effectiveness and Biomechanics of Spinal Orthoses in The Treatment of Adolescent Idiopathic Scoliosis (AIS) |
12 |
|
8 |
Goldberg et al [31] |
Adolescent Idiopathic Scoliosis- The Effect of Brace Treatment On The Incidence of Surgery |
12 |
|
9 |
Karol [32] |
Effectiveness of Bracing in Male Patients with Idiopathic Scoliosis |
12 |
|
10 |
Chase, Bader and Houghton [33] |
The Biomechanical Effectiveness of The Boston Brace in The Management of Adolescent Idiopathic Scoliosis |
11 |
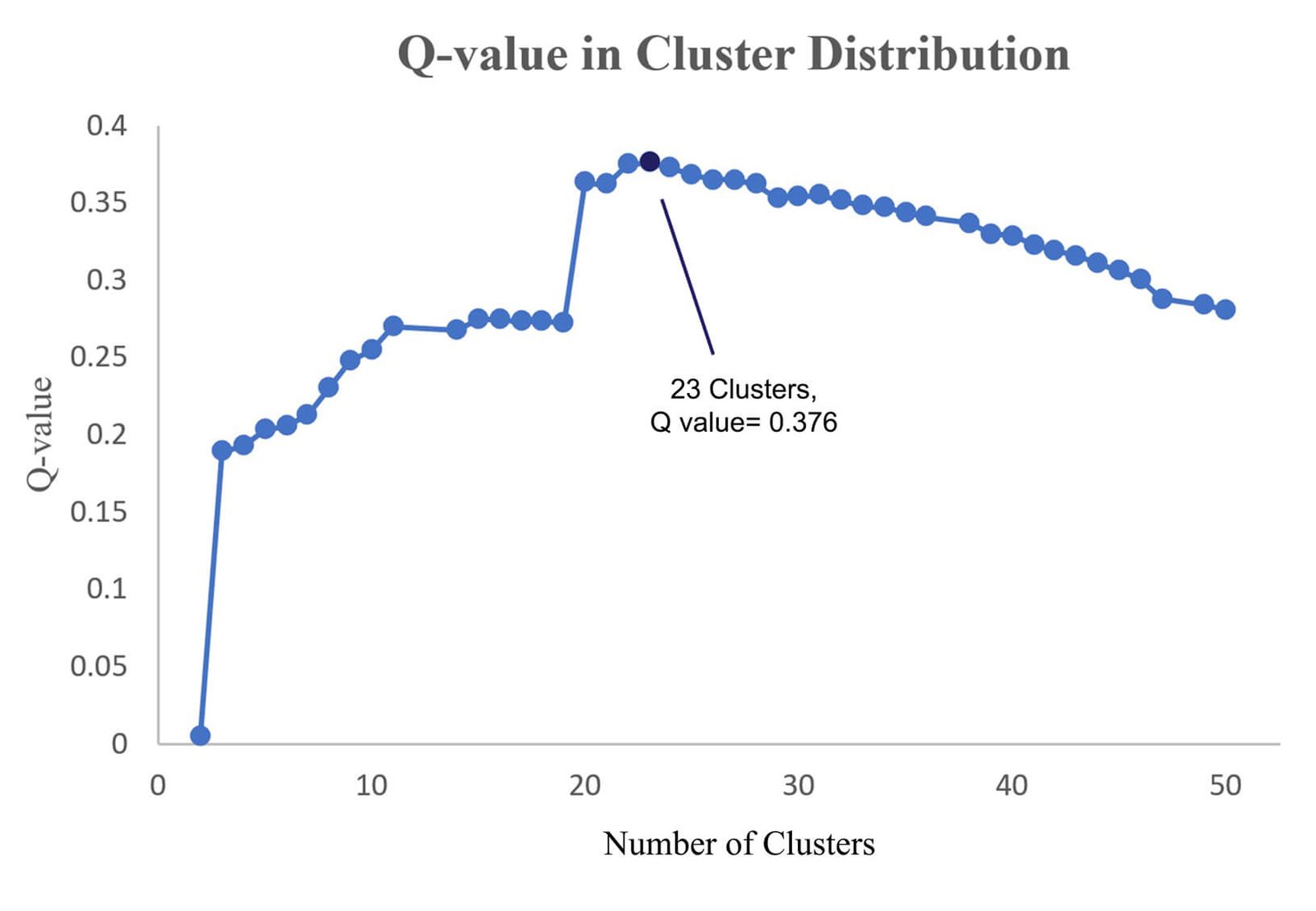
Figure 6: Q-values of Girvan-Newman clusters.
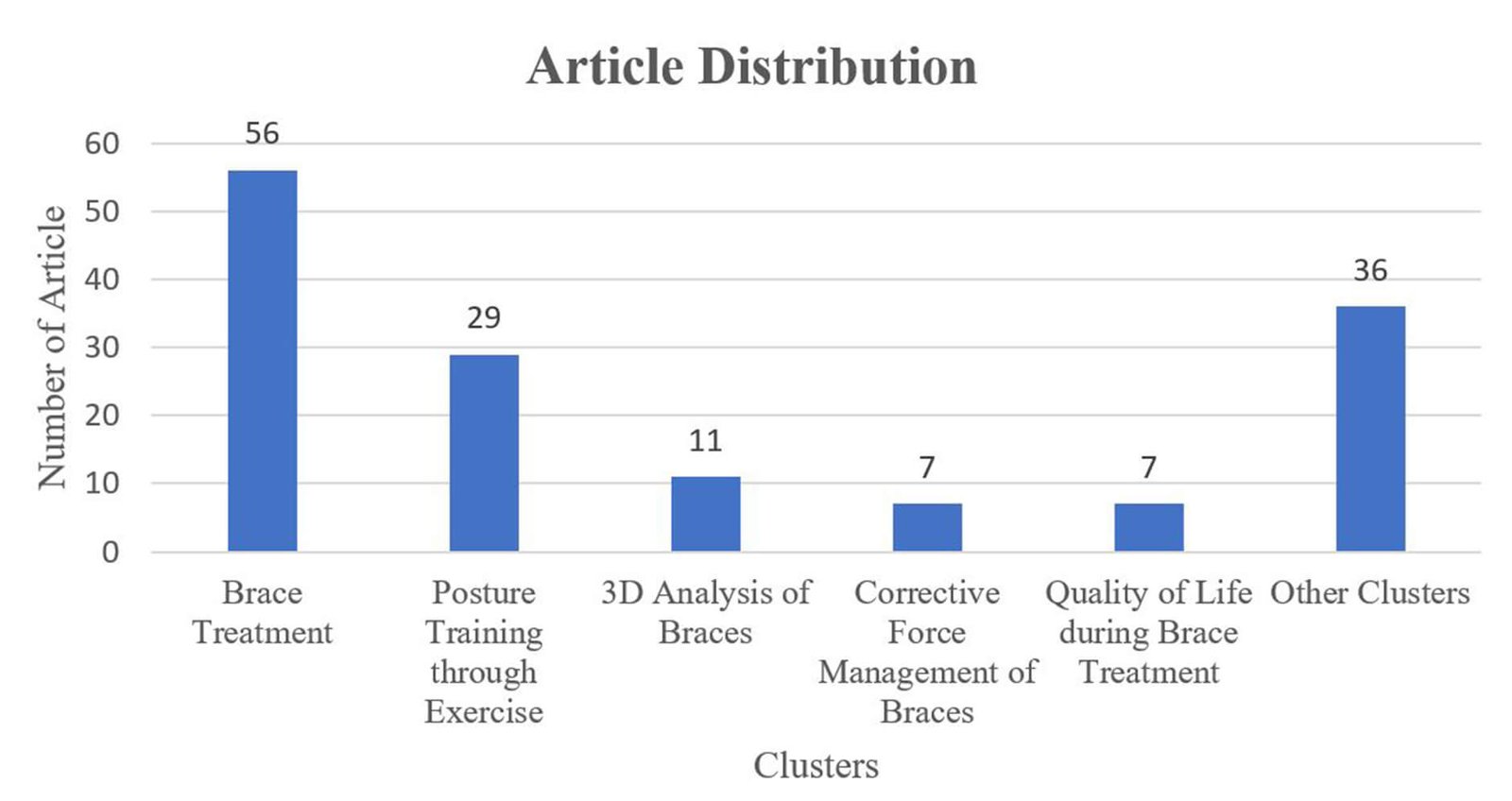
Figure 7: Classification of research clusters.
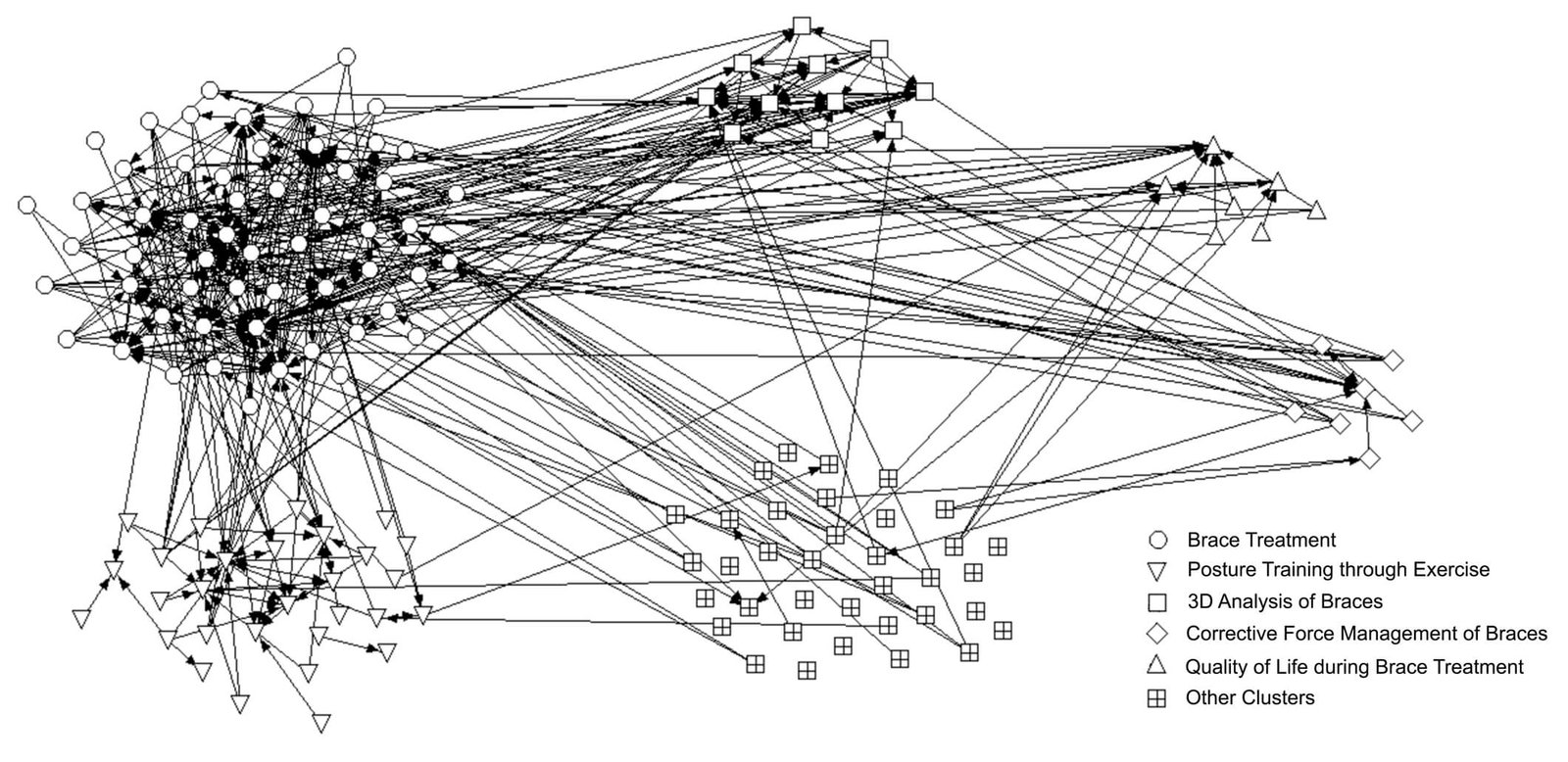
Figure 8: Citation network structure of the shortlisted articles.
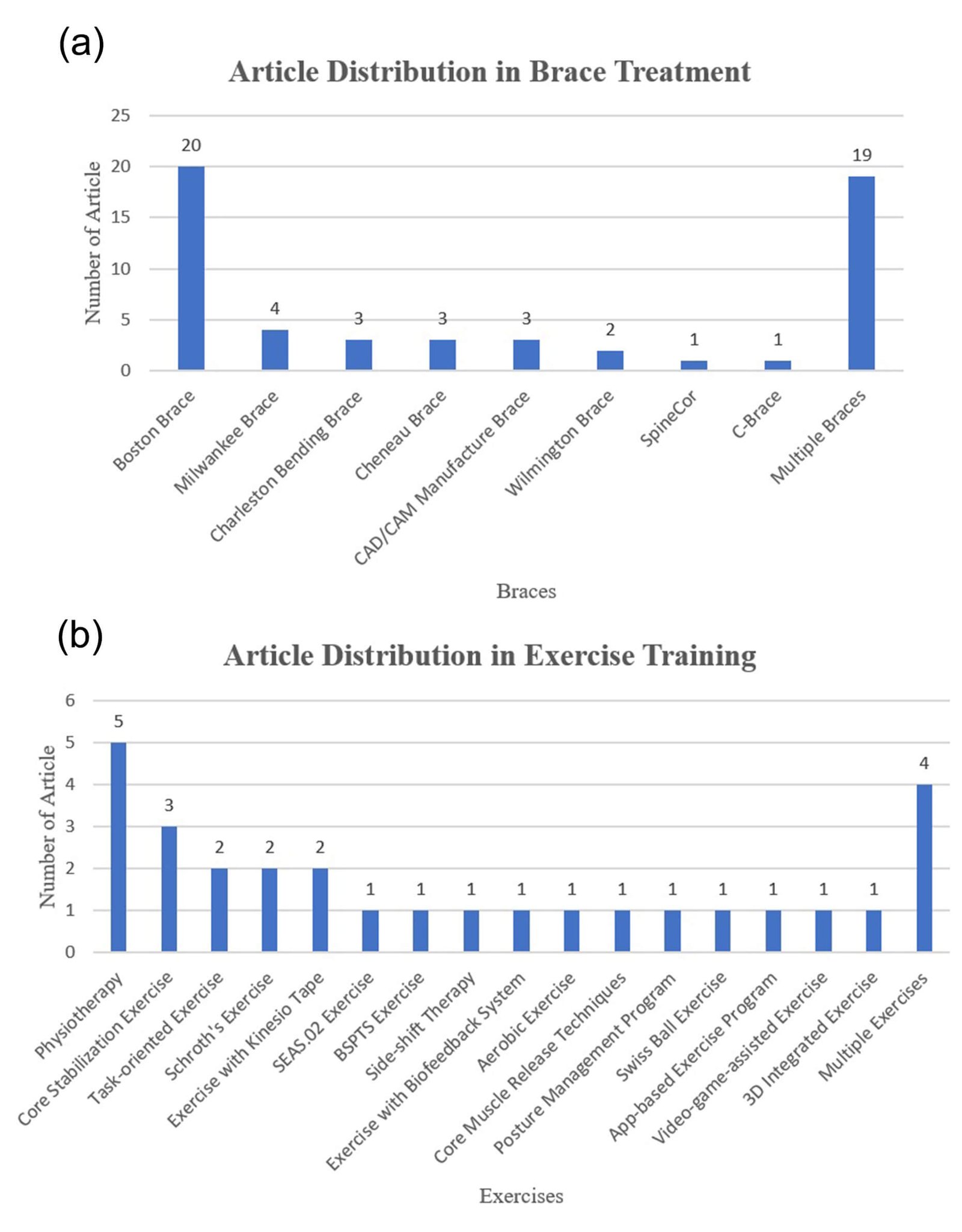
Figure 9: Article distribution of two main clusters. (a) Distribution within brace treatment. (b) Distribution within posture training through exercise.
Discussion
Treatments such as exercise and bracing might be the only means other than surgical procedures for patients to monitor and control their curve progression of spine [7]. Surgery, such as spinal fusion, can be avoided only for those with a small Cobb angle. In general, hard braces are commonly used as an effective treatment for AIS [39]. It is not surprising that the number of recent studies on noninvasive treatment of AIS has been rapidly increasing, demonstrating the interest of scholars in this particular area. However, Robinson and Woggon and Wiley et al. noted that most AIS patients who undergo bracing treatment are prone to depression due to the awkward and bulky appearance of the rigid brace and related discomfort, even if brace treatment is deemed an effective nonsurgical treatment for AIS [40, 41]. To cope with the variability of nonsurgical treatment, the lack of consensus regarding bracing options and the uncertainties about certain exercises, a comprehensive review is needed to summarize previous studies on noninvasive treatment for AIS and identify potential research opportunities. In this review, the popularity of nonsurgical options is also evident from the citation score. As shown in (Table 2), the 10 most influential papers focusing on nonsurgical treatment were listed according to their LCS. In fact, these articles were cited multiple times by other academics worldwide in the same field. Almost all had a GCS score of 100 or higher, especially Rowe et al. Lonstein and Carlson, Nachemson et al. which had the 3 highest GCSs of 485, 372 and 212, respectively [24, 30, 31].
However, these results do not mean that there are sufficient research studies in this field. As (Figure 4) shows, there is a lack of meta-analyses. Furthermore, 7 of the 10 articles with the highest LCSs focused on bracing as a treatment for AIS; they examined the Boston brace and the Milwaukee brace, which are rigid braces [27, 32]. Although some papers examined semi-rigid and flexible braces, posture training through exercise or other nonsurgical treatments, none of the most influential papers focused on these areas [24, 25]. This finding shows researchers' relative lack of interest in or neglect of these areas of study. Meanwhile, the research clusters shown in (Figures 6 & 8) also lend support to this argument. This might be due to the wide use of rigid braces to treat AIS and their proven effectiveness in halting spinal curvature progression. The research cluster of brace treatment was clearly the largest research domain, with 35 articles on rigid braces (62.5%) and only 2 articles on non-rigid braces (3.6%). Hard orthoses comprised the subject of not only the majority of the studies in the largest cluster (brace treatment) but also the other three main research clusters (corrective force management of braces, 3D analysis of braces, and quality of life during brace treatment). This significant difference in the number of studies and research efforts show the research gap in studies of non-rigid braces.
In addition, only a few research studies have examined posture training for AIS (19.9%), and almost 70% of the mentioned exercises were proposed by only one article. This situation reveals the potential for research regarding posture training through exercise and other nonsurgical treatments aside from non-rigid braces, in particular, semi-rigid and flexible braces, exercise with biofeedback systems, posture management programs and other exercises, which had only been studied in one article in the WoS database.
Although the bracing effect of rigid braces was supported by most articles in the brace cluster, they also pointed out the limitations of such rigid orthoses, in which 41.7% of these 24 articles represented patient compliance of brace treatment and tightness of brace were the largest concerns that might affect the brace effectiveness [42-44]. There were still a few evidences on these areas, even if temperature loggers and battery-powered microcomputer systems were applied to cope with such limitations [43, 44]. It is vital to have a better understanding and solution of treatment compliance, brace design, and the physical effects (such as skin irritation) of nonsurgical treatments for AIS, which also represent the shortcomings of most current orthoses. These areas comprise further research opportunities for scholars. Like all other research papers, there are limitations in this review article. First, some of the more recently published articles have yet to appear on the academic radar due to a low citation impact. Having a citation impact requires time [45]. Second, only one database, the WoS, and English articles were taken into consideration for the sample. Therefore, relevant papers might have been omitted from this review study, which consequently may have affected the results. Moreover, there could have been negative citations (i.e., citing others to criticize them), which cause citation polarity and bias the results, although this is not a substantial problem in most cases [19].
Conclusion
This systematic review, which uses a CNA, examined the noninvasive treatment of AIS based on a sample of 146 articles. By using HistCite, the article distribution was examined in terms of publication year, name of journal, type of article and country/region of the authors. More importantly, five main research clusters were classified through the CNA: brace treatment, posture training through exercise, corrective force management of braces, 3D analysis of braces and quality of life during brace treatment. Brace treatment as a topic comprised the largest cluster of research studies, and almost all of the articles on this topic focused on rigid braces. In contrast, semi-rigid and flexible braces, exercise using a biofeedback system, posture management programs and other types of posture training exercises that had only one included article in this database have not been the focus of academia. These areas represent the research gaps in this field. Future studies could consider conducting meta-analyses of nonsurgical treatments for AIS; improving the patient compliance and brace design; or developing a flexible brace, such as semi-rigid brace, for AIS with both spinal corrective functions and materials that are perceived to be comfortable to the wearer.
Acknowledgement
We thank Mrs. Qing-Rui Li from the Institute of Pathology and Southwest Cancer Center, Southwest Hospital, Third Military Medical University, Chongqing, China for her work on sample collection.
Contributors
SHW, JY and KYCL: conception and study design. SHW and JY: acquisition and data, data analysis, and drafting of the manuscript. SHW and KYCL: statistical analysis. JY, KYCL, KMCC, JPYC, KYHK, KLY and SPN: critical revision of the manuscript for important intellectual content, technical or material support, and supervision.
Article Info
Article Type
Review of LiteraturePublication history
Received: Sat 28, Dec 2019Accepted: Fri 10, Jan 2020
Published: Thu 30, Jan 2020
Copyright
© 2023 Joanne Yip. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SSG.2020.01.01
Figures & Tables
Table 1: Article distribution: top 5 countries.
|
Country |
Number of included articles |
|
USA |
35 |
|
Canada |
25 |
|
China |
17 |
|
Italy |
8 |
|
France |
7 |
Table 2: Articles with the highest LCS.
|
Rank |
Author |
Title |
LCS |
|
1 |
Nachemson et al [25] |
Effectiveness of Treatment with A Brace in Girls Who Have Adolescent Idiopathic Scoliosis- A Prospective, Controlled-Study Based On Data From The Brace Study of The Scoliosis-Research-Society |
37 |
|
2 |
Emans et al [26] |
The Boston Bracing System for Idiopathic Scoliosis- Follow-up Results in 295 Patients |
27 |
|
3 |
Lonstein and Carlson [27] |
The Prediction of Curve Progression in Untreated Idiopathic Scoliosis During Growth |
19 |
|
4 |
Noonan et al [28] |
Use of The Milwaukee Brace for Progressive Idiopathic Scoliosis |
19 |
|
5 |
Rowe et al [24] |
A Meta-Analysis of The Efficacy of Non-Operative Treatments for Idiopa{Muthukrishnan, 2010 #221}thic Scoliosis |
18 |
|
6 |
Bunnell [29] |
The Natural-History of Idiopathic Scoliosis Before Skeletal Maturity |
14 |
|
7 |
Wong et al [30] |
Effectiveness and Biomechanics of Spinal Orthoses in The Treatment of Adolescent Idiopathic Scoliosis (AIS) |
12 |
|
8 |
Goldberg et al [31] |
Adolescent Idiopathic Scoliosis- The Effect of Brace Treatment On The Incidence of Surgery |
12 |
|
9 |
Karol [32] |
Effectiveness of Bracing in Male Patients with Idiopathic Scoliosis |
12 |
|
10 |
Chase, Bader and Houghton [33] |
The Biomechanical Effectiveness of The Boston Brace in The Management of Adolescent Idiopathic Scoliosis |
11 |
References
- Reamy BV, Slakey JB (2001) Adolescent idiopathic scoliosis: review and current concepts. Am Fam Physician 64: 111-116. [Crossref]
- Scoliosis Research Society Terminology Committee (1976) A Glossary of Scoliosis Terms. Spine 1: 57-58.
- Weiss HR, Negrini S, Rigo M, Kotwicki T, Hawes MC et al. (2006) Indications for conservative management of scoliosis (guidelines). Scoliosis 1: 5. [Crossref]
- Sun X, Wu T, Liu Z, Zhu Z, Qian B et al. (2013) Osteopenia predicts curve progression of adolescent idiopathic scoliosis in girls treated with brace treatment. J Pediatr Orthop 33: 366-371. [Crossref]
- Asher M, Burton D (2006) Adolescent idiopathic scoliosis: natural history and long term treatment effects. Scoliosis 1: 2. [Crossref]
- Dewald RL (2003) Spinal deformities: the comprehensive text. Thieme.
- Dolan AL, Donnelly JM, Spratt FK, Weinstein LS (2007) Professional Opinion Concerning the Effectiveness of Bracing Relative to Observation in Adolescent Idiopathic Scoliosis. J Pediatr Orthop 27: 270-276. [Crossref]
- USC Center for Spinal Surgery (2005) Scoliosis, Children’s spine surgery. USC Center for Spinal Surgery.
- Coillard C, Leroux MA, Zabjek KF, Rivard C (2003) SpineCor–a non-rigid brace for the treatment of idiopathic scoliosis: post-treatment results. Eur Spine J 12: 141-148. [Crossref]
- Chan WY, Yip J, Yick KL, Ng SP, Lu L et al. (2018) Mechanical and Clinical Evaluation of a Shape Memory Alloy and Conventional Struts in a Flexible Scoliotic Brace. Ann Biomed Eng 46: 1194-1205. [Crossref]
- Wong MS, Cheng JCY, Lam TP, Ng BKW, Sin SW et al. (2008) The effect of rigid versus flexible spinal orthosis on the clinical efficacy and acceptance of the patients with adolescent idiopathic scoliosis. Spine 33: 1360-1365. [Crossref]
- Bulthuis GJ, Veldhuizen AG, Nijenbanning G (2008) Clinical effect of continuous corrective force delivery in the non-operative treatment of idiopathic scoliosis: a prospective cohort study of the TriaC-brace. Eur Spine J 17: 231-239. [Crossref]
- Margaret Slota D (2018) AACN Core Curriculum for Pediatric High Acuity, Progressive, and Critical Care Nursing. Springer .
- Colicchia C, Strozzi F (2012) Supply chain risk management: a new methodology for a systematic literature review. Supply Chain Management. An International Journal 17: 403-418.
- Ngai EWT, Moon KKL, Riggins FJ, Yi CY (2007) RFID research: An academic literature review (1995–2005) and future research directions. Int J Production Econ 112: 510-520.
- Hummon NP, Dereian P (1989) Connectivity in a citation network: The development of DNA theory. Social Networks 11: 39-63.
- Wetzstein A, Feisel E, Hartmann E, Benton Jr W (2018) Uncovering the supplier selection knowledge structure: A systematic citation network analysis from 1991 to 2017. J Purchasing Supply Management.
- Apriliyanti ID, Alon I (2017) Bibliometric analysis of absorptive capacity. Int Business Rev 26: 896-907.
- Pilkington A, Meredith J (2009) The evolution of the intellectual structure of operations management—1980–2006: A citation/co-citation analysis. J Operations Management 27: 185-202.
- Borgatti SP, Everett MG, Freeman LC (2002) Ucinet for Windows: Software for Social Network Analysis. Analytic Technologies, Harvard, MA.
- Chen P, Redner S (2010) Community structure of the physical review citation network. J Informetrics 4: 278-290.
- Girvan M, Newman ME (2002) Community structure in social and biological networks. Proc Natl Acad Sci U S A 99: 7821-7826. [Crossref]
- Newman MEJ, Girvan M (2004) Finding and evaluating community structure in networks. Physical Review E - Statistical, Nonlinear, and Soft Matter Physics. 69: 1-16.
- Rowe DE, Bernstein SM, Riddick MF, Adler F, Emans JB et al. (1997) A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J Bone Joint Surg Am 79: 664-674. [Crossref]
- Bunnell WP (1986) The natural-history of idiopathic scoliosis before skeletal maturity. Spine (Phila Pa 1976) 11: 773-776. [Crossref]
- Chase AP, Bader DL, Houghton GR (1989) The biomechanical effectiveness of the Boston brace in the management of adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 14: 636-642. [Crossref]
- Emans JB, Kaelin A, Bancel P, Hall JE, Miller ME (1986) The Boston bracing system for idiopathic scoliosis - Follow-up results in 295 patients. Spine (Phila Pa 1976) 11: 792-801. [Crossref]
- Goldberg CJ, Moore DP, Fogarty EE, Dowling FE (2001) Adolescent idiopathic scoliosis - The effect of brace treatment on the incidence of surgery. Spine (Phila Pa 1976) 26: 42-47. [Crossref]
- Karol LA (2001) Effectiveness of bracing in male patients with idiopathic scoliosis. Spine (Phila Pa 1976) 26: 2001-2005. [Crossref]
- Lonstein J, Carlson J (1984) The prediction of curve progression in untreated idiopathic scoliosis during growth. J Bone Joint Surg-Am 66: 1061-1071. [Crossref]
- Nachemson AL, Peterson LE (1995) Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis - A prospective, controlled-study based on data from the brace study of the scoliosis-research-society. J Bone Joint Surg-Am 77: 815-822. [Crossref]
- Noonan KJ, Weinstein SL, Jacobson WC, Dolan LA (1996) Use of the Milwaukee brace for progressive idiopathic scoliosis. J Bone Joint Surg Am 78: 557-567. [Crossref]
- Wong MS, Mak AFT, Luk KDK, Evans JH, Brown B (2000) Effectiveness and biomechanics of spinal orthoses in the treatment of adolescent idiopathic scoliosis (AIS). Prosthet Orthot Int 24: 148-162. [Crossref]
- O'Neill PJ, Karol LA, Shindle MK, Elerson EE, Brintzenhofeszoc KM et al. (2005) Decreased orthotic effectiveness in overweight patients with adolescent idiopathic scoliosis. J Bone Joint Surg-Am 87: 1069-1074. [Crossref]
- Wong MS, Cheng JCY, Wong MW, So SF (2005) A work study of the CAD/CAM method and conventional manual method in the fabrication of spinal orthoses for patients with adolescent idiopathic scoliosis. Prosthet Orthot Int 29: 93-104. [Crossref]
- Wong MS, Cheng JCY, Lo KH (2005) A comparison of treatment effectiveness between the CAD/CAM method and the manual method for managing adolescent idiopathic scoliosis. Prosthet Orthot Int 29: 105-111. [Crossref]
- Cobetto N, Aubin CE, Parent S, Clin J, Barchi S et al. (2016) Effectiveness of braces designed using computer-aided design and manufacturing (CAD/CAM) and finite element simulation compared to CAD/CAM only for the conservative treatment of adolescent idiopathic scoliosis: a prospective randomized controlled trial. Eur Spine J 25: 3056-3064. [Crossref]
- Eshraghi A, Maroufi N, Sanjari MA, Saeedi H, Keyhani MR et al. (2013) Effect of Milwaukee brace on static and dynamic balance of female hyperkyphotic adolescents. Prosthet Orthot Int 37: 76-84. [Crossref]
- Trobisch P, Suess O, Schwab F (2010) Idiopathic scoliosis. Dtsch Arztebl Int 107: 875-883. [Crossref]
- Robinson GR, Woggon J (2011) Postural Rehab/Forensic Practices/Personal Injury-The Impact of Scoliosis on the People Living with it and their Families. Am Chiropractor 33: 14.
- Wiley JW, Thomson JD, Mitchell TM, Smith BG, Banta JV (2000) Effectiveness of the Boston brace in treatment of large curves in adolescent idiopathic scoliosis. Spine (Phila Pa 1976) 25: 2326-2332. [Crossref]
- Korovessis P, Zacharatos S, Koureas G, Megas P (2007) Comparative multifactorial analysis of the effects of idiopathic adolescent scoliosis and Scheuermann kyphosis on the self-perceived health status of adolescents treated with brace. Eur Spine J 16: 537-546. [Crossref]
- Lou E, Hill DL, Raso JV, Moreau MJ, Mahood JK (2005) Smart orthosis for the treatment of adolescent idiopathic scoliosis. Med Biol Eng Comput 43: 746-750. [Crossref]
- Lou E, Raso JV, Hill DL, Durdle NG, Mahood JK et al. (2002) The daily force pattern of spinal orthoses in subjects with adolescent idiopathic scoliosis. Prosthet Orthot Int 26: 58-63. [Crossref]
- Fahimnia B, Sarkis J, Davarzani H (2015) Green supply chain management: A review and bibliometric analysis. Int J Production Economics 162: 101-114.