Neuroendocrine Small-Cell Carcinoma of the Gallbladder: Case Report
A B S T R A C T
Gallbladder neuroendocrine carcinoma is a very rare entity, accounting for <0.2% of all neuroendocrine tumours [1]. Of the cases described in the literature, the initial presentation is usually locally advanced or even with disseminated disease [2]. In this paper we report the case of a 43-year-old female patient with an incidental diagnosis of gallbladder neuroendocrine carcinoma. Although clinical presentation is the most common, it is a very rare condition that poses a therapeutic and prognostic challenge.
Keywords
Gallbladder tumors, neuroendocrine tumors, small-Cell neuroendocrine carcinoma
Introduction
Primary Neuroendocrine Tumors (NET) of the gallbladder are rare, and while well-differentiated NETs have an indolent course and overall good prognosis, poorly differentiated neuroendocrine carcinomas (NEC) have a poor outcome [3]. Histological types of gallbladder NET can be divided in well-differentiated carcinoid tumors, small-cell carcinomas (grade 1) and large-cell neuroendocrine carcinomas (grade 2) and mixed adeno-neuroendocrine carcinomas (MANEC) [3, 4]. Of these types, carcinoid tumors have a more favorable course where small-cell neuroendocrine and undifferentiated carcinomas have a poor prognosis [5-7]. In this case report we pretend to illustrate the presentation, diagnosis, evolution and outcome of a small-cell NEC of the gallbladder and the struggle to optimize the treatment to this aggressive form of NET.
Case Presentation
A 43-year-old female presented to the emergency department with abdominal pain, localized in the right upper quadrant for the last 24 hours with lumbar irradiation. She referred accompanying vomit and nausea. Denied any other accompanying symptoms like fever, jaundice and/or constitutional symptoms. No previously relevant medical history. On physical examination, the patient had abdominal tenderness in the right hypochondrium and a positive Murphy’s sign. Laboratory studies showed a mild leucocytosis and a non-elevated C reactive protein (CRP). An abdominal ultrasound revealed a regular hepatic contour with a 5cm hyperechogenic nodular formation on segment 5, suggestive of hemangioma; no dilatation of the biliary tract and a distended gallbladder with multiple calculi, with parietal thickening and pain on instrumental compression.
Based on these findings we proposed a surgical approach for a laparoscopic cholecystectomy that was consented by the patient. Intraoperatively we found the gallbladder with parietal wall thickening and surrounded by inflammatory tissue, confirming the clinical suspicion of acute cholecystitis. The surgery was otherwise uneventful, and the patient was discharged at the third post-operative day. Histopathological analysis revealed a small-cell NEC of the gallbladder with serous infiltration and perforation, lymphovascular and perineural invasion and metastatic disease in the cystic lymph node: pTNM T3N1Mx. The patient underwent a thoraco-abdomino-pelvic CT scan, which revealed a hepatic lesion with 8cm-diameter in segment 4 with arterial enhancement, consistent with a secondary location. No other suspicious lesions where identified (Figure 1).
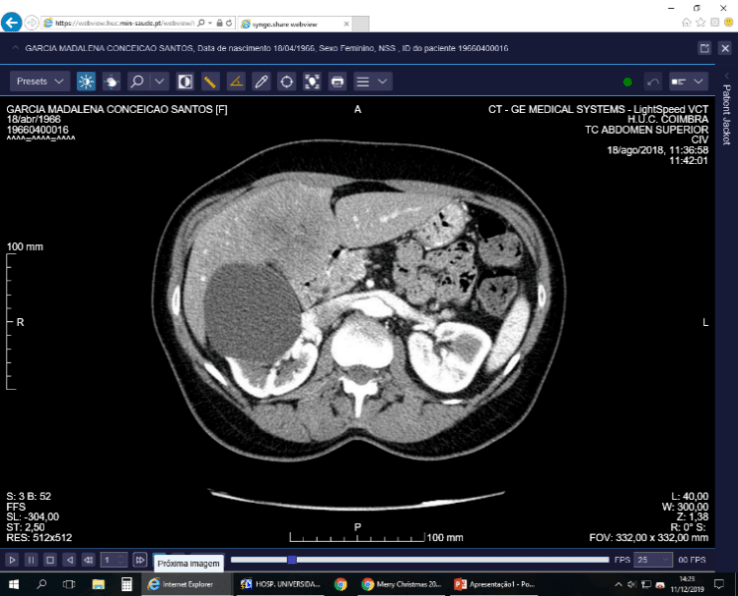
Figure 1: Initial assessment after the histopathology diagnosis, showcasing liver metastasis.
An FDG-PET was also performed and revealed a hepatic secondary location in segment 4, corresponding to the same site on the CT-scan, and metastatic lymphatic invasion involving the hepatic hilum. The patient was proposed for systemic chemotherapy. Besides QT, disease progression occurred and reevaluation with FDG-PET after 6 weeks of QT showed a progressing liver metastasis and the appearance of multiple bone metastasis, with the patient dying at 9 months after the initial diagnosis. (Figure 2).

Figure 2: Post QT assessment that reveals the progressing of liver infiltration.
Discussion
This case illustrates the rapid evolution of the NEC of the gallbladder, with a poor prognosis, short-term survival and little to no response to chemotherapy. Gallbladder carcinomas prognosis is dependent not only on local staging but also of the histological type – so adenocarcinomas and other well-differentiated tumors have a better outcome than small-cell neuroendocrine and other poorly differentiated tumors. The literature compares most NET of the gallbladder behavior to gallbladder adenocarcinoma, especially the poorly differentiated ones, poor prognosis, usually with late-stage presentation. In the specific case of small-cell neuroendocrine carcinoma, the few cases described in the literature – the behavior of these tumors seems to be even more aggressive than the gallbladder adenocarcinoma with shorter survival after diagnosis and even worst response to chemotherapy. So, although surgical radical resection is the paramount treatment it is rarely doable or of any clinical benefit at all.
Conclusion
Gallbladder neuroendocrine carcinomas are initially at an advanced stage and do not respond to chemotherapy regimens. Rarely with the possibility of radical surgical therapy and poor prognosis. The median survival is 4-6 months despite the therapeutic measures instituted [8]. Nevertheless, a recognition of a neuroendocrine type carcinoma is important to evaluate prognosis and also to prevent and treat other paraneoplastic syndromes as well as a possible different chemotherapy scheme.
Article Info
Article Type
Research ArticlePublication history
Received: Thu 19, Dec 2019Accepted: Wed 01, Jan 2020
Published: Sat 11, Jan 2020
Copyright
© 2023 Carolina V. Canhoto. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.01.03
Figures & Tables
References
- Mezi S, Petrozza V, Schillaci O, La Torre V, Cimadon B et al. (2011) Neuroendocrine tumors of the gallbladder: a case report and review of the literature. J Med Case Rep 5: 334. [Crossref]
- Liu W, Chen W, Chen J, Hong T, Li B (2019) Neuroendocrine carcinoma of gallbladder: a case series and literature review. Eur J Med Res 24: 8. [Crossref]
- Komminoth P, Arnold R, Capella C, Klimstra DS, Kloppel G et al. (2010) Neuroendocrine neoplasms of the gallbladder and extrahepatic bile ducts. In: Bosman FT, Carneiro F, Hruban RH, Theise ND, editors. World health organization of tumours: pathology and genetics of tumours of the digestive system. 4th ed. Lyon (France): International Agency for Research on Cancer (IARC) 274-276.
- Iype S, Mirza TA, Propper DJ, Bhattacharya S, Feakins RM et al. (2009) Neuroendocrine tumours of the gallbladder: three cases and a review of the literature. Postgrad Med J 85: 213-218. [Crossref]
- Noske A, Pahl S (2006) Combined adenosquamous and large-cell neuroendocrine carcinoma of the gallbladder. Virchows Arch 449: 135-136. [Crossref]
- Carriaga MT, Henson DE (1995) Liver, gallbladder, extrahepatic bile ducts, and pancreas. Cancer 75: 171-190. [Crossref]
- Fujii H, Aotake T, Horiuchi T, Chiba Y, Imamura Y et al. (2001) Small cell carcinoma of the gallbladder: a case report and review of 53 cases in the literature. Hepatogastroenterology 48: 1588-1593. [Crossref]
- Kamboj M, Gandhi JS, Gupta G, Sharma A, Pasricha S et al. (2015) Neuroendocrine Carcinoma of Gallbladder: A Series of 19 Cases with Review of Literature. J Gastrointest Cancer 46: 356-364. [Crossref