Journals
Minimally invasive technique for mixed-type asymmetric thoracic deformity
A B S T R A C T
Mixed-type asymmetric thoracic deformity has two malformations in left to right parallel arrangement. Although the deformity is regarded as a simple addition of pectus carinatum and pectus excavatum, the sandwich procedure will not bring ideal results. We designed a minimally invasive technique using one or two metal bars to correct the protrusion and depression at the same time, and our preliminary clinical experience shows a satisfactory result.
K E Y W O R D S
asymmetric thoracic deformity, minimally invasive, operation
Introduction
Mixed-type deformity of the anterior chest wall refers to the deformity with both protrusion and depression (Fig 1) [1]. We designed a special operation that used one or two metal bars to correct the protrusion and depression at the same time, which is different from other procedures.
Technique
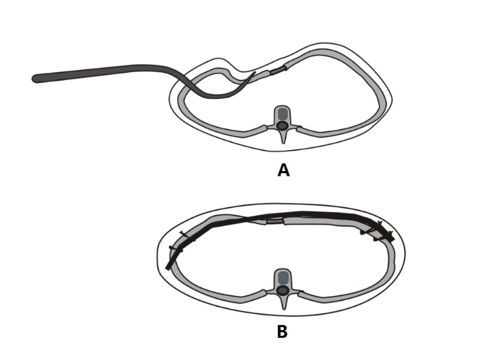
The patient is in supine position, with double upper arms at the abduction position. Two incisions are made on both sides of the chest wall respectively, located near the midaxillary line, roughly at the plane of lowest part of the depression (also the top part of the protrusion). The length of incisions is 2-3cm. On the depression side, the subcutaneous tissue and muscle are incised and retracted, and 3-4 ribs arroud the depression are exposed. An intercostal incision is made just beneath the deepest rib, so that the chest cavity can be entered. After the deepest rib is retracted upwards, a long bar introducer is inserted into the chest cavity and passed through the upper intercostal space near the sternum to the surface of bony structures [Fig 2A]. A tunnel is made to the direction of the center line, from the front of the sternum to the other side. On the protrusion side of the chest wall, a tunnel is made beneath the pectoralis major muscle, which is located at the most severe part of protrusion and connected to the tunnel on the opposite side of chest wall. The bar introducer is placed in the tunnel, then, a bar is pulled into the tunnel. The bar is located on the surface of the bony structure on the protrusion side, while beneath the deepest rib on the depression side [Fig 2B]. In this way, the protrusion is flattening, and the depression is supported at the same time. After the two ends of bar are fixed firmly, the incision is sutured, and the operation is accomplished ultimately.
For patients with small area of lesions, one bar should be enough. If the lesion area is large, or for adult patients after puberty, as the bone is hard, two bars should be used. When tow bars are used, the position of the bars should be evenly arranged according to the shape of lesion. The walking pathes of the bars are similar to that of one bar.
Figures

Comment
Mixed-type deformity of the anterior chest wall is composed of two single malformations [1, 2]. If only one malformation is treated, another will get serious, therefore, the sandwich procedure is introduced [2]. For mixed-type asymmetric thoracic deformity, since the lesions are in parallel arrangement from right to left, the sandwich procedure cannot achieve good results.
Generally speaking, this special deformity can be classified as 2A type of pectus excavatumm by Park’s classification, meanwhile, it can also be classified as the asymmetric type of pectus carinatum [2, 3]. For the former, Park used a special surgical treatment, but it was still Nuss procedure. Although the author claimed good results could be obtained, this procedure doesn't seem to be a good option. If it is regarded as the asymmetry type of pectus carinatum, minimally invasive surgery for pectus carinatum seem to be useful, but just like Nuss procedure, it can make the contralateral malformation more obvious. In order to make a satisfactory result, some traditional surgical methods such as modified Ravitch procedure was used, but the larger trauma and longer incisions are obviously not ideal choices [3].
The advantage of our method is that two combined malformations can be treated at one time. Since the operation is completed only by two small incisions, it also has the advantage of minimally invasive operation.
In our technique, the shape of the bar is the key factor for the operation. We adopt an asymmetric design in our technique. On the protrusion side, the bar radian should be small, so that the protrusion can be flatten; On the depression side, the radian should be large, so that the depression can be supported effectively.
From the mechanical point of view, since the forces acting on the depressed chest wall are derived from the elastic reaction force of the flattened chest wall, it is conceivable that the fixation of the bar is very important for such an operation. If not firm, it is easy to cause surgery failure. In order to obtain an ideal fixation effect, we use double steel wires to fix the bar directly to the two ribs just beneath the bar [Fig 2B]. This method is proved to be an ideal fixation procedure.
Article Info
Article Type
Short CommunicationPublication history
Received 24 May, 2018Accepted 4 June, 2018
Published 15 June, 2018
Copyright
© 2018 Wenlin Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.10.31487/j.SCR.2018.02.003
Author Info
Corresponding author
Wenlin WangDepartment of Chest Wall Surgery, Guangdong Second General Provincial Hospital, Guangzhou 510317, P.R.China
Figures & Tables
References
1. Akkas Y, Kocer B, Peri NG (2016) A new technique for mixed-type pectus carinatum: modified Onen method. Asian Cardiovasc Thorac Ann 24: 227-230. [Crossref]
2. Park HJ, Kim KS (2016) The sandwich technique for repair of pectus carinatum and excavatum/carinatum complex. Ann Cardiothorac Surg 5: 434–439 [Crossref]
3. Cortés-Julián G, Bushra-Nuritu HB, Buenfil-Fuentes R, Merino Rajme J (2017) Modified Ravitch procedure for left Poland syndrome combined with pectus excavatum. Ann Thorac Surg 104: 337-339. [Crossref]