Micronutrient Malnutrition – A Glimpse on the Current Strategies and Future Prospects
A B S T R A C T
The inadequacy of micronutrients, namely essential vitamins and minerals in the human diet, manifests a wide range of moderate to serious health concerns collectively known as micronutrient malnutrition. It affects half of the global population, and food-based strategies such as balanced diet, supplementation and food fortification are effective. The balanced diet and dietary supplementation are desirable and sustainable; however, their efficacy is uncertain due to the required demands to improve dietary habits. Interestingly, food fortification – addition of micronutrients to processed foods – supplies micronutrients without the need to alter eating habits and unquestionably stands out as a systematic approach to moderate the statistical rise in micronutrient malnutrition. On the other hand, biofortification – plant breeding and/or genetic engineering – is a convenient and sustainable strategy with myriad possibilities to augment micronutrients status that could endure through generations. These approaches coupled with meticulously organized innovative policies and a competent food value chain will indeed aid in addressing the micronutrient deficiency toward building a productive and efficient generation.
Keywords
Micronutrient malnutrition, Food-based strategies, Balanced diet, Supplementation, Food fortification, Biofortification
Micronutrient Malnutrition
Malnutrition, an imbalance in the body due to excessive intake or deficiency of energy/nutrients, can be broadly classified as macro- and micro-nutrient malnutrition. Due to significant contribution to the energy build-up, only the former gained attention from the policymakers, government officials and general public. However, micro-nutrient malnutrition cannot be disregarded. Micro-nutrients, though require only in trace amounts, aid in human metabolism, body’s homeostasis and physiological functioning [1]. They are critical to prevent a host of diseases and their deficiency i) increases morbidity and poor pregnancy, ii) hampers early childhood growth with impaired mental and physical development, and iii) affects work productivity, to name a few [2].
Micronutrients are a group of organic substances (fat- and water-soluble vitamins) and inorganic minerals. Among the 51 vitamins and minerals identified to maintain health, calcium, phosphorous, magnesium, iodine, iron, zinc, copper, sulfur, manganese, chromium, fluorine, selenium, molybdenum, and vitamins A, C, D, E, K, and B, a total of 19 nutrients, are considered essential toward physical and mental development and immune system functioning [3]. Their Recommended Dietary Allowances (RDA), an average daily dietary requirement that signifies the sufficient micronutrient intake of healthy individuals, have been developed (Table 1) to address the physiological demands. Toward this end, diets with optimally dense and bioavailable micronutrients are essential; micronutrient density is the amount of micronutrients present in a given food per calorie, whilst bioavailability signifies the total absorbable fraction of ingested nutrient.
Global Burden
Micronutrients deficiency afflicts nearly half of the world population [4]. They often prevail as part of the malnutrition cycle and could as well be coupled with macro-nutrient malnutrition. The widespread iron, vitamin A, iodine, folate and zinc deficiencies are highlighted in the following sections.
Table 1: Recommended Dietary Allowances (RDA) of essential micronutrients along
with prevalence and health consequences [64].
|
Nutrient |
Pregnancy |
Lactation |
Child |
Teens |
Adults |
Prevalence |
Consequences |
|||||||||
|
|
1-3 y |
4-8 y |
9-13 |
14-18 |
19-50 |
51-70 |
>70y |
|||||||||
|
Boy |
Girl |
Boy |
Girl |
M |
F |
M |
F |
M |
F |
|||||||
|
Vitamins |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vitamin A (µg) |
770 |
1,300 |
300 |
400 |
600 |
600 |
900 |
700 |
900 |
700 |
900 |
700 |
900 |
700 |
Very common |
Night blindness, dry eyes, impaired immunities, infertility, throat and
chest infections |
|
Vitamin C (mg) |
85 |
120 |
15 |
25 |
45 |
45 |
75 |
65 |
90 |
75 |
90 |
75 |
90 |
75 |
Uncommon |
Scurvy, bleeding gums, dry, rough and bumpy skin, bruising, poor immunity |
|
Vitamin D (µg) |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
20 |
20 |
Common |
Rickets, Osteomalacia, muscle pain, hair loss, fatigue |
|
Vitamin E (mg) |
15 |
19 |
6 |
7 |
11 |
11 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
Very rare |
Digestive disorders, impaired immunity, sterility |
|
Vitamin K (µg) |
90* |
90* |
30* |
55* |
60* |
60* |
75* |
75* |
120* |
90* |
120* |
90* |
120* |
90* |
Common in infants; |
Excessive bleeding, inadequate absorption, dark stool |
|
Vitamin B1 (mg) |
1.4 |
1.4 |
0.5 |
0.6 |
0.9 |
0.9 |
1.2 |
1.0 |
1.2 |
1.1 |
1.2 |
1.1 |
1.2 |
1.1 |
Uncommon in adults |
Beriberi, cardiac failure, irritability, fatigue |
|
Vitamin B2 (mg) |
1.4 |
1.6 |
0.5 |
0.6 |
0.9 |
0.9 |
1.3 |
1.0 |
1.3 |
1.1 |
1.3 |
1.1 |
1.3 |
1.1 |
Uncommon |
Cheilosis, sore tongue and throat, metabolic disorders |
|
Vitamin B3 (mg) |
18 |
17 |
6 |
8 |
12 |
12 |
16 |
14 |
16 |
14 |
16 |
14 |
16 |
14 |
Uncommon |
Pellagra, swelling of mucous membrane, dementia, digestive disorders |
|
Vitamin B5 (mg) |
6* |
7* |
2* |
3* |
4* |
4* |
5* |
5* |
5* |
5* |
5* |
5* |
5* |
5* |
Uncommon@ |
Fatigue, insomnia, often coupled with other vitamin deficiencies |
|
Vitamin B6 (mg) |
1.9 |
2.0 |
0.5 |
0.6 |
1.0 |
1.0 |
1.3 |
1.2 |
1.3 |
1.3 |
1.7 |
1.5 |
1.7 |
1.5 |
Rare |
Dermatitis, microcytic anemia, fissures |
|
Vitamin B12 (µg) |
2.6 |
2.8 |
0.9 |
1.2 |
1.8 |
1.8 |
2.4 |
2.4 |
2.4 |
2.4 |
2.4# |
2.4# |
2.4# |
2.4# |
Rare |
Pernicious anemia, sore tongue, neurological problems |
|
Biotin (µg) |
30* |
35* |
8* |
12* |
20* |
20* |
25* |
25* |
30* |
30* |
30* |
30* |
30* |
30* |
Uncommon@ |
Digestive issues, hair loss, skin rashes, muscle aches and fatigue, mood
changes |
|
Folic acid (µg) |
600 |
500 |
150 |
200 |
300 |
300 |
400 |
400 |
400 |
400 |
400 |
400 |
400 |
400 |
Uncommon |
Fatigue, gray hair, mouth sores, tongue
swelling, growth problems, pale skin, anemia |
|
Minerals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Calcium (mg) |
1,000 |
1,000 |
700 |
1,000 |
1,300 |
1,300 |
1,300 |
1,300 |
1000 |
1000 |
1000 |
1200 |
1,200 |
1,200 |
Common |
Weak and fragile bones, muscle spasms, memory loss, seizures |
|
Chromium (µg) |
30* |
45* |
11* |
15* |
25* |
21* |
35* |
24* |
35* |
25* |
30* |
20* |
30* |
20* |
Uncommon |
Diabetes (roles in insulin-action), weight loss, increment in cholesterol
level, increased risk of heart attacks |
|
Copper (µg) |
1000 |
1,300 |
340 |
440 |
700 |
700 |
890 |
890 |
900 |
900 |
900 |
900 |
900 |
900 |
Rare |
Easy bone breakage, easy bruising, fatigue, pale skin, poor growth, skin
inflammation, skin sores, unexplained muscle soreness, always feeling cold |
|
Fluoride (mg) |
3* |
3* |
0.7* |
1* |
2* |
2* |
3* |
3* |
4* |
3* |
4* |
3* |
4* |
3* |
Uncommon |
Dental caries, weak and fragile bones |
|
Iodine (µg) |
220 |
290 |
90 |
90 |
120 |
120 |
150 |
150 |
150 |
150 |
150 |
150 |
150 |
150 |
Very common |
Goiter, hypothyroidism, pregnancy issues |
|
Iron (mg) |
27 |
9 |
7 |
10 |
8 |
8 |
11 |
15 |
8 |
18 |
8 |
8 |
8 |
8 |
Very common |
Anemia, fatigue and dizziness, pale skin, palpitation, shortness of
breath, cold hands and feet, tongue swelling, brittle nails |
|
Magnesium (mg) |
350 |
320 |
80 |
130 |
240 |
240 |
410 |
360 |
420 |
320 |
420 |
320 |
420 |
320 |
Uncommon@ |
Decreased appetite, weakness, muscle cramps, osteoporosis, heart
diseases, asthma |
|
Manganese (mg) |
2.0* |
2.6* |
1.2* |
1.5* |
1.9* |
1.6* |
2.2* |
1.6* |
2.3* |
1.8* |
2.3* |
1.8* |
2.3* |
1.8* |
Rare |
Poor bone health, digestive issues, low fertility |
|
Molybdenum (µg) |
50 |
50 |
17 |
22 |
34 |
34 |
43 |
43 |
45 |
45 |
45 |
45 |
45 |
45 |
Very rare |
Impaired dental health |
|
Phosphorus (mg) |
700 |
700 |
460 |
500 |
1,250 |
1,250 |
1,250 |
1,250 |
700 |
700 |
700 |
700 |
700 |
700 |
Rare |
Fatigue, muscle weakness, anxiety, formation of large pulp chambers in
teeth |
|
Selenium (µg) |
60 |
70 |
20 |
30 |
40 |
40 |
55 |
55 |
55 |
55 |
55 |
55 |
55 |
55 |
Rare |
Infertility, myopathy, muscle weakness, fatigue, mental fog, hair loss,
weakened immunity |
|
Zinc (mg) |
11 |
12 |
3 |
5 |
8 |
8 |
11 |
9 |
11 |
8 |
11 |
8 |
11 |
8 |
Common |
Diarrhea, loss of appetite, rashes around mouth, nose and anus, decreased
alertness, unhealing of wounds, lack of alertness, infertility |
Vitamin A as Retinol Activity Equivalents (RAE); Vitamin D as
Cholecalciferol; Vitamin E as α-tocopherol; Vitamin B3 as Niacin Equivalents (NE); Folic acid as Dietary Folate Equivalent (DFE).
* Denotes to the Average
Intake (AI), which is different from RDA. That is calculated from an Estimated
Average Requirement (EAR). AI is established when there is no sufficient
scientific evidence to develop EAR.
# Refers to suggested
intake through supplementation, as age group >50 may have malabsorption of Vitamin B12.
@Vitamin B5 deficiency
often prevails with alcoholism and digestive disorders; Biotin deficiency is
common mostly in vegan community; Magnesium deficiency is common in people with
diabetics, gastrointestinal diseases and alcoholism.
Legend: M: Male, F: Female
I Iron
Iron regulates several biochemical processes such as electron transfer reactions, gene regulation, binding and transport of oxygen, and regulation of cell growth and differentiation. Its deficiency contributes to anemia. It is essential for fetal growth and development, and thus iron demand is high during pregnancy and any shortage onsets the intrauterine growth restriction, premature delivery, low birth weight and postpartum depression, to name a few [5]. South Asia and Sub-Saharan Africa account for the highest anemia prevalence in pregnant women and pre-school children of 47.7 and 55.1 %, and 45.8 and 59.9%, respectively [6, 7].
II Vitamin A
Vitamin A is essential for vision. It also controls human health, growth, immune system function and reproduction. Vitamin A deficiency (VAD) is associated with several non-communicable and infectious diseases [8]. The prevalence of low serum retinol concentration of <0.70 µmol/L contributes to VAD, and during 2009 it was estimated that 190 million pre-school children and 19.1 million pregnant women were at risk [9]. Furthermore, 5.17 million pre-school children and 9.75 million pregnant women were found to be affected by night blindness [9]. Night blindness is an early symptom of VAD, and prolonged deficiency of Vitamin A leads to serious multiorgan, multisymptomatic and potentially fatal diseases.
III Iodine
Dietary iodine supports the thyroid hormone production that is required for the overall metabolism. Its demand further escalates during pregnancy for bone and brain development of fetus, and inadequacy results in irreversible neurological complications leading to mental retardation in offspring, commonly known as Iodine Deficiency Disorder (IDD). Mainly pregnant women and pre-school children are at a greater risk. Due to government efforts and several intervention programmes, IDD is decreasing around the world, as evidenced by lower goiter rates and urinary iodine concentration [10]. However, globally more than 2 billion people are still combating IDD, as only a few countries reached full iodine adequacy.
IV Zinc
The global prevalence of zinc deficiency is poorly known because of the issues concerning the assessment of zinc status by biomarkers. Consequently, zinc deficiency data are predominantly based on the availability of zinc in the food supply and estimated daily intake [11]. Predictably, half of the global population is at the risk of low intake of zinc and the majority (61%) are from the developing countries [12]. Around 17.3% of the world’s population is projected to have zinc deficiency, with the highest figures coming from Africa (23.9%) and Asia (19.4%) [13].
V Folate
The folic acid, also known as Vitamin B9, deficiency has long been known to have adverse health effects, including megaloblastic anemia and neural tube defect (NTD) [14]. Though global data is not available, only a few small and local surveys have been carried out on folate insufficiency threshold concentration indicators like serum folate (<10 nmol/L) and red blood cells (RBC) folate (<340 nmol/L) [15]. It usually exists in people with high alcoholism, malabsorptive disorders, pregnant and child-bearing women [16].
VI Multiple Micro-Nutrient Malnutrition
Micronutrient deficiencies are commonly driven by poor-quality diets. Despite the fact that the aforementioned deficiencies are the most common, multiple micronutrient deficiencies often coexist [17]. Their prevalence, coupled with data limitation, make it difficult to plan and adopt appropriate interventions. In this regard, global hidden hunger indices databases developed based on i) stunting, iron deficiency anemia, VAD, and IDD and ii) Disability-adjusted life years (DALY) offer valuable insights to prioritize target populations and plan effective strategies [18].
Current Efforts
The United Nations (UN) considers malnutrition, in all its forms, as the most urgent and pervasive challenge and has been actively pursuing options to eradicate malnutrition throughout the world. During 2016-2025, the UN Decade of Action on Nutrition has been developed with an objective to transform the prevalent food system (food production, processing and distribution) to deliver healthy and nutritious foods along with reducing food inequalities [19]. The UN specialized agencies – Food and Agriculture Organization (FAO) and World Health Organization (WHO) – have taken charge on collaborative efforts with World Food Programme (WFP) and International Fund for Agricultural Development (IFAD) to promote innovative food system strategies and to improve overall nutrient density and bioavailability. Furthermore, one of the Sustainable Development Goals (SDGs) of Zero Hunger set by the UN focuses on ending all forms of malnutrition through improved nutrition and sustainable agriculture by 2030.
Strategies to Mitigate Micronutrient Malnutrition
Chronic micronutrient malnutrition is a diet-related concern that cannot be reverted but could be fixed through food-based strategies such as i) balanced diet, ii) supplementation, iii) food fortification and iv) biofortification (Figure 1). The approaches are aimed at immediate and/or long-term responses toward controlling and preventing micronutrient deficiency. In order for them to be successful, they ought to be cost-effective, sustainable and comply with the culturally acceptable norms. A synergistic collaboration between the potential consumer, food industry and government along with relevant organizations and nutritional initiatives is critical for the long-term success. The outcome, certainly, helps to retard the micronutrient malnutrition and in-turn wanes dependency on the healthcare system.
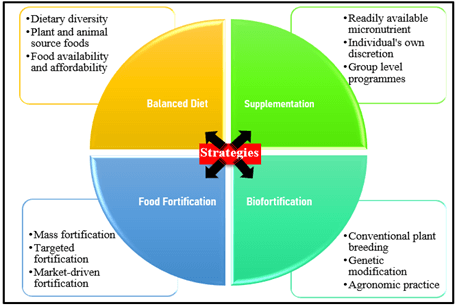
Figure 1: Food-based strategies to mitigate micronutrient malnutrition.
I Balanced Diet
Whether it is to guard against chronic health problems or to promote growth or even to bestow energy on a daily basis, a balanced diet is vital. It encompasses foods of diverse commodities to furnish essential micronutrients. Structuring and consuming such diets could not only prevent the macro- and micro-nutrient malnutrition but also a gamut of non-communicable diseases. Implementation of a balanced diet is quite challenging, however, due to continuously changing lifestyles and consumers propensity toward processed foods. A key component of a balanced diet is the dietary diversification. Diets with variety of foods across and within food groups – grains, protein, dairy, vegetables, fruits and oils – overshadow the possible limiting factors and ensure adequate intake of essential nutrients. Indeed, dietary diversification correlates positively with nutritional wellbeing. For example, the anthropometric status of children of 1-3 years significantly associates with the consumption of different food groups [20]. However, infants and young children (6-23 months) from several low- and middle-income countries are deprived of reaching the minimum dietary diversity accentuating their dependence on non-nutrient and starchy foods [21].
More importantly, balanced diet of individuals is largely shaped by their cognizance toward nutrient content, availability, affordability and preparation time, in addition to religious taboos and preferences. Animal-based foods are regarded as easily accessible sources of multiple bioavailable nutrients and their consumption might replenish the deprived nutrients [22]. In developing countries, their consumption is still a concern predominantly due to non-availability and non-affordability, despite some signs of improvement, and thus these regions appears to be hotspots of micronutrient malnutrition [23]. Furthermore, with a substantial emphasis on the balanced diet but without a pragmatic application creates dietary inequalities across countries and through rural and affluent communities. In this regard, implementation, monitoring and timely evaluation of novel strategies with teams of specialists from agriculture, nutrition, public health, epidemiology and psychology sectors coupled with proper budgeting are in need.
II Supplementation
Supplements are available in a variety of forms, such as capsules, tablets, syrups, powders and gels. FDA recommends them as ‘foods’, owing to their intended purpose [24]. Supplements use, indeed, is effective to address micronutrient deficiency and eventually to prevent chronic health issues [25-27]. They could be consumed at individual discretion. They improve the micronutrient status at a significant pace and confer health, especially for the high-risk individuals, specified groups, and targeted community.
For example, iron supplementation to anemic pregnant women reduces preterm births and decreases the prevalence of congenital abnormalities in newborns [25]. Further addition of folic acid, cuts-down the risks of low birth weight, maternal anemia and iron deficiency [28]. Similarly, Vitamin A supplementation in 6-59-month old kids curtails the child mortality due to measles and diarrhea [26]. Supplementation is the most widely applied intervention strategy and has proven to be effective in controlling VAD. On the other hand, iodine supplementation, different from fortification, is not recommended unless a particular individual is at a severe risk of iodine deficiency. Its intake, through iodine tables and iodized oil, during pregnancy lowers the birth defects, premature delivery and infant mortality [29]. Supplementation, however, needs to be considered as complimentary to food fortification and bio-fortification. Its improper dosing leads to toxicity, and thus appropriate quantity and frequency of dosing are critical for gaining envisioned benefits [30].
III Food Fortification
Food fortification is the deliberate act to increase essential micronutrients to improve the nutritional quality of foods and public health with minimal risks [31]. There are three types of food fortification based on the application and scope: mass fortification, targeted fortification, and market-driven (or commercial) fortification. Mass fortification is the addition of micronutrients to commonly consumed foods such as cereals, condiments and milk. It is usually mandated by the government. The most effective example is salt iodization, practiced globally since 1924, which not only decreased the prevalence of goiter, cretinism and iodine deficiency but also improved national efficiency [32]. On the other hand, targeted fortification is designed for specific sub-groups such as infants and young children, pregnant and lactating women and vulnerable micronutrient deficient communities [4]. Iron fortification in complementary foods to restrain anemia in children and folic acid in flours to abate Neural Tube Defects are a couple of successful examples [33, 34]. Market-driven fortification is a business-oriented initiative that particularly increases sales of a specific food product and profitability. Such voluntary act offers food manufacturers to develop micronutrient fortified foods within the regulatory standards [35]. For example, fortification of ready-to-eat breakfast cereals and dairy products escalates the intake of fortified foods and increases the micronutrient levels [36]. Multi-nutrient fortification is also practiced to address multifarious health concerns [37-39].
In order for the food fortification to be effective, the selected micronutrient needs to be delivered using compatible and convenient food vehicles. These cargos facilitate reaching out a larger cohort of vulnerable populations in an efficient and inexpensive manner without altering the dietary patterns. Generally, any food could be fortified, but cereals are the most accomplished ones as they are staple foods, especially in the hotspot regions [40-42]. In addition, oils, milk and dairy products, noodles, beverages and chocolates have also been exploited [31, 43-47]. Most importantly, bioavailability and compatibility dictate the micronutrient choice. For example, iron fortification demands ferrous and ferric forms, retinyl palmitate for Vitamin A fortification, potassium iodide for iodine fortification and zinc oxide for zinc fortification [4, 48-50]. Overall, food fortification unquestionably stands out as a systematic approach to develop micronutrient-dense foods and by far the most cost-effective strategy [51]. The process demands technical expertise, however, and requires sophisticated paraphernalia [35]. More importantly, rigorous regulations for food producers, educational programmes and the availability of fortified foods at a reasonable price are critical for its successful implementation.
IV Biofortification
‘Biofortification’, or Biological Fortification, is to enrich micronutrient content of agriculture produce through plant breeding or genetic engineering [52]. It could also be described based on agronomic practices and the use of mineral-rich fertilizers, but this ideology is being disregarded due to intrinsic environmental and cost issues. Most importantly, biofortification is a one-time investment and yields micronutrient dense crops that could endure for generations. This multiplier aspect justifies clearly for it to be a food-based strategy and be regarded as the most sustainable and long-term means to address the micronutrient deficiency.
Conventional plant breeding is the process of identifying and incorporating the desirable traits of one crop into another in order to develop improved varieties in the progeny. It is normally called crossbreeding or hybridization and is prevalent for ages. Over the years, plant breeders have acclimatized with more scientific exposures and nutrient-dense crops with those of low-level nutrients [53]. Such efforts resulted in the production of Iron beans, Iron-zinc sorghum, Iron pearl millet, Vitamin-A Maize, Vitamin-A Orange Flesh Sweet Potato, Vitamin-A Yellow cassava, Zinc rice and Zinc Wheat, to name a few [54]. For example, Orange Flesh Sweet Potatoes yield up to 1371 RAE/100 kcal of Vitamin A [55]. Their use for daily foods namely baby foods and jam and bread aid to combat vitamin A deficiency [56, 57]. Similarly, consumption of iron-pearl millet meal increases the iron content in children and iron-beans intake elevates the iron level in haemoglobin, serum ferritin and total body iron in women [58, 59].
On the other hand, modern biotechnology involves bioengineering or genome editing with which a specific genetic donor organism trait is shared with the recipient [60]. Upon acceptance, the recipient shows the characteristics of the donor and remains eternal. This scientific advancement allows transfer of specific genes to staple crops to produce sustainable micronutrient foods and will certainly lower the micronutrient deficiency. For example, transferring the β-carotene synthesizing ability of daffodil plant to rice results in β-carotene rice, also known as golden rice [61, 62]. One another successful invention is the Vitamin-A banana [63].
Overall, plant breeding and genetic engineering boost the nutritional content of staple crops and succor for sustained and long-term means of nutrition delivery toward improving human health. However, micronutrient-rich crops warrant judicial distribution with considerations such as, i) biofortified foods must have a measurable impact on improving human nutrition and should meet the Recommended Daily Allowances, ii) micronutrients must be bioavailable and should not wither during storage and processing conditions, iii) consumers should be able to accept the biofortified crops without changing their established dietary habits, iv) genetic manipulation must sustain, if not increase, the productivity and v) biofortified crops should be amenable to food safety protocols and environmental concerns. Overall, biofortification is deemed to support the scientific community to develop breeds that could be readily acceptable by farmers toward abolishing micronutrient malnutrition and warrants further research.
Micronutrient Malnutrition: From Reality to Nullity
Health is the highest human value of all time. This perception of individual’s health is indebted to a healthy and nutritious diet. However, malnutrition exists in every society, and alarmingly, the micronutrient malnutrition, which demands the design and development of appropriate strategies from individuals through the government level to address it effectively. In this perspective, four strategies – balanced diet, supplementation, food fortification and biofortification – are exemplified toward alleviating micronutrient malnutrition. The first is to follow a balanced diet – blend of plant and animal-based commodities – that is often an ideal solution to supply all-inclusive nutrients. On the other hand, supplementation – capsules, tablets and syrups – is a quick and significant way of conferring micronutrients to high-risk individuals and groups. The food fortification – addition of nutrients to foods – is to make regularly consumed foods as nutritionally dense without altering the existing dietary pattern, which undeniably serves as the best approach to cover a wider population. Biofortification – incrementing the nutritional value of crops – is the panacea of micronutrient challenges to not only resolve micronutrient unavailability but also to supply vital nutrients through generations.
Indeed, these strategies have challenges. Balanced diet takes time to show the measurable impact, whilst supplementation is more for targeted groups with a specific mineral deficiency. Similarly, demand for monitory aspects precludes widespread applicability of fortified foods, mainly in low-income communities. Though biofortification appears to be the nascent alternative; there are many yet-to-be realized concerns for large-scale utility. Overall, food-based strategies supported through meticulously organized innovative policies and a competent food value chain will aid in addressing the micronutrient deficiency and building a productive and efficient current and future generation.
Acknowledgement
Support from the USDA National Institute for Food and Agriculture (SD00H648-18) is greatly appreciated.
Article Info
Article Type
Research ArticlePublication history
Received: Thu 08, Jul 2021Accepted: Sat 24, Jul 2021
Published: Fri 06, Aug 2021
Copyright
© 2023 Srinivas Janaswamy. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JFNM.2021.02.02
Figures & Tables
Table 1: Recommended Dietary Allowances (RDA) of essential micronutrients along
with prevalence and health consequences [64].
|
Nutrient |
Pregnancy |
Lactation |
Child |
Teens |
Adults |
Prevalence |
Consequences |
|||||||||
|
|
1-3 y |
4-8 y |
9-13 |
14-18 |
19-50 |
51-70 |
>70y |
|||||||||
|
Boy |
Girl |
Boy |
Girl |
M |
F |
M |
F |
M |
F |
|||||||
|
Vitamins |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vitamin A (µg) |
770 |
1,300 |
300 |
400 |
600 |
600 |
900 |
700 |
900 |
700 |
900 |
700 |
900 |
700 |
Very common |
Night blindness, dry eyes, impaired immunities, infertility, throat and
chest infections |
|
Vitamin C (mg) |
85 |
120 |
15 |
25 |
45 |
45 |
75 |
65 |
90 |
75 |
90 |
75 |
90 |
75 |
Uncommon |
Scurvy, bleeding gums, dry, rough and bumpy skin, bruising, poor immunity |
|
Vitamin D (µg) |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
20 |
20 |
Common |
Rickets, Osteomalacia, muscle pain, hair loss, fatigue |
|
Vitamin E (mg) |
15 |
19 |
6 |
7 |
11 |
11 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
15 |
Very rare |
Digestive disorders, impaired immunity, sterility |
|
Vitamin K (µg) |
90* |
90* |
30* |
55* |
60* |
60* |
75* |
75* |
120* |
90* |
120* |
90* |
120* |
90* |
Common in infants; |
Excessive bleeding, inadequate absorption, dark stool |
|
Vitamin B1 (mg) |
1.4 |
1.4 |
0.5 |
0.6 |
0.9 |
0.9 |
1.2 |
1.0 |
1.2 |
1.1 |
1.2 |
1.1 |
1.2 |
1.1 |
Uncommon in adults |
Beriberi, cardiac failure, irritability, fatigue |
|
Vitamin B2 (mg) |
1.4 |
1.6 |
0.5 |
0.6 |
0.9 |
0.9 |
1.3 |
1.0 |
1.3 |
1.1 |
1.3 |
1.1 |
1.3 |
1.1 |
Uncommon |
Cheilosis, sore tongue and throat, metabolic disorders |
|
Vitamin B3 (mg) |
18 |
17 |
6 |
8 |
12 |
12 |
16 |
14 |
16 |
14 |
16 |
14 |
16 |
14 |
Uncommon |
Pellagra, swelling of mucous membrane, dementia, digestive disorders |
|
Vitamin B5 (mg) |
6* |
7* |
2* |
3* |
4* |
4* |
5* |
5* |
5* |
5* |
5* |
5* |
5* |
5* |
Uncommon@ |
Fatigue, insomnia, often coupled with other vitamin deficiencies |
|
Vitamin B6 (mg) |
1.9 |
2.0 |
0.5 |
0.6 |
1.0 |
1.0 |
1.3 |
1.2 |
1.3 |
1.3 |
1.7 |
1.5 |
1.7 |
1.5 |
Rare |
Dermatitis, microcytic anemia, fissures |
|
Vitamin B12 (µg) |
2.6 |
2.8 |
0.9 |
1.2 |
1.8 |
1.8 |
2.4 |
2.4 |
2.4 |
2.4 |
2.4# |
2.4# |
2.4# |
2.4# |
Rare |
Pernicious anemia, sore tongue, neurological problems |
|
Biotin (µg) |
30* |
35* |
8* |
12* |
20* |
20* |
25* |
25* |
30* |
30* |
30* |
30* |
30* |
30* |
Uncommon@ |
Digestive issues, hair loss, skin rashes, muscle aches and fatigue, mood
changes |
|
Folic acid (µg) |
600 |
500 |
150 |
200 |
300 |
300 |
400 |
400 |
400 |
400 |
400 |
400 |
400 |
400 |
Uncommon |
Fatigue, gray hair, mouth sores, tongue
swelling, growth problems, pale skin, anemia |
|
Minerals |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Calcium (mg) |
1,000 |
1,000 |
700 |
1,000 |
1,300 |
1,300 |
1,300 |
1,300 |
1000 |
1000 |
1000 |
1200 |
1,200 |
1,200 |
Common |
Weak and fragile bones, muscle spasms, memory loss, seizures |
|
Chromium (µg) |
30* |
45* |
11* |
15* |
25* |
21* |
35* |
24* |
35* |
25* |
30* |
20* |
30* |
20* |
Uncommon |
Diabetes (roles in insulin-action), weight loss, increment in cholesterol
level, increased risk of heart attacks |
|
Copper (µg) |
1000 |
1,300 |
340 |
440 |
700 |
700 |
890 |
890 |
900 |
900 |
900 |
900 |
900 |
900 |
Rare |
Easy bone breakage, easy bruising, fatigue, pale skin, poor growth, skin
inflammation, skin sores, unexplained muscle soreness, always feeling cold |
|
Fluoride (mg) |
3* |
3* |
0.7* |
1* |
2* |
2* |
3* |
3* |
4* |
3* |
4* |
3* |
4* |
3* |
Uncommon |
Dental caries, weak and fragile bones |
|
Iodine (µg) |
220 |
290 |
90 |
90 |
120 |
120 |
150 |
150 |
150 |
150 |
150 |
150 |
150 |
150 |
Very common |
Goiter, hypothyroidism, pregnancy issues |
|
Iron (mg) |
27 |
9 |
7 |
10 |
8 |
8 |
11 |
15 |
8 |
18 |
8 |
8 |
8 |
8 |
Very common |
Anemia, fatigue and dizziness, pale skin, palpitation, shortness of
breath, cold hands and feet, tongue swelling, brittle nails |
|
Magnesium (mg) |
350 |
320 |
80 |
130 |
240 |
240 |
410 |
360 |
420 |
320 |
420 |
320 |
420 |
320 |
Uncommon@ |
Decreased appetite, weakness, muscle cramps, osteoporosis, heart
diseases, asthma |
|
Manganese (mg) |
2.0* |
2.6* |
1.2* |
1.5* |
1.9* |
1.6* |
2.2* |
1.6* |
2.3* |
1.8* |
2.3* |
1.8* |
2.3* |
1.8* |
Rare |
Poor bone health, digestive issues, low fertility |
|
Molybdenum (µg) |
50 |
50 |
17 |
22 |
34 |
34 |
43 |
43 |
45 |
45 |
45 |
45 |
45 |
45 |
Very rare |
Impaired dental health |
|
Phosphorus (mg) |
700 |
700 |
460 |
500 |
1,250 |
1,250 |
1,250 |
1,250 |
700 |
700 |
700 |
700 |
700 |
700 |
Rare |
Fatigue, muscle weakness, anxiety, formation of large pulp chambers in
teeth |
|
Selenium (µg) |
60 |
70 |
20 |
30 |
40 |
40 |
55 |
55 |
55 |
55 |
55 |
55 |
55 |
55 |
Rare |
Infertility, myopathy, muscle weakness, fatigue, mental fog, hair loss,
weakened immunity |
|
Zinc (mg) |
11 |
12 |
3 |
5 |
8 |
8 |
11 |
9 |
11 |
8 |
11 |
8 |
11 |
8 |
Common |
Diarrhea, loss of appetite, rashes around mouth, nose and anus, decreased
alertness, unhealing of wounds, lack of alertness, infertility |
Vitamin A as Retinol Activity Equivalents (RAE); Vitamin D as
Cholecalciferol; Vitamin E as α-tocopherol; Vitamin B3 as Niacin Equivalents (NE); Folic acid as Dietary Folate Equivalent (DFE).
* Denotes to the Average
Intake (AI), which is different from RDA. That is calculated from an Estimated
Average Requirement (EAR). AI is established when there is no sufficient
scientific evidence to develop EAR.
# Refers to suggested
intake through supplementation, as age group >50 may have malabsorption of Vitamin B12.
@Vitamin B5 deficiency
often prevails with alcoholism and digestive disorders; Biotin deficiency is
common mostly in vegan community; Magnesium deficiency is common in people with
diabetics, gastrointestinal diseases and alcoholism.
Legend: M: Male, F: Female
References
1. Shergill Bonner R
(2013) Micronutrients. Paediatr Child Health 23: 331-336.
2. Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis
M et al. (2008) Maternal and child undernutrition: global and regional
exposures and health consequences. Lancet 371: 243-260. [Crossref]
3. Kennedy G, Nantel
G, Shetty P (2003) The scourge of "hidden hunger": global dimensions
of micronutrient deficiencies. Food Nutr Agric 32: 8-16.
4. Allen L, de Benoist
B, Dary O, Hurrell R (2006) Guidelines on food fortification with
micronutrients. WHO, FAO UN 341.
5. Georgieff MK (2020)
Iron deficiency in pregnancy. Am J Obstet Gynecol 223: 516-524. [Crossref]
6. World Bank (2016)
Prevalence of anemia among pregnant women (%).
7. World bank (2019)
Prevalence of anemia among children (% of children under 5).
8. Semba RD (1994)
Vitamin A, immunity, and infection. Clin Infect Dis 19: 489-499. [Crossref]
9. World Health
Organization (2009) Global prevalence of vitamin A deficiency in populations at
risk 1995-2005: WHO Global Database on Vitamin A Deficiency. Geneva, World
Health Organization.
10. Huhtaniemi I, Martini L (2018) Iodine deficiency. Encyclopedia
Endocrine Diseases,
2nd ed 2018: 512-523.
11. Wessells KR, Brown
KH (2012) Estimating the global prevalence of zinc deficiency: results based on
zinc availability in national food supplies and the prevalence of stunting. PLoS
One 7: e50568. [Crossref]
12. Akhtar S (2013)
Zinc status in South Asian populations--an update. J Health Popul Nutr
31: 139-149. [Crossref]
13. Bailey RL, West KP,
Black RE (2015) The epidemiology of global micronutrient deficiencies. Ann
Nutr Metab 66: 22-33. [Crossref]
14. Bergman JEH, Otten
E, Verheij JBGM, de Walle HEK (2016) Folic acid supplementation influences the
distribution of neural tube defect subtypes: A registry-based study. Reprod
Toxicol 59: 96-100. [Crossref]
15. Bailey LB, Stover
PJ, McNulty H, Fenech MF, Gregory JF 3rd et
al. (2015) Biomarkers of Nutrition for Development-Folate Review. J
Nutr 145: 1636S-1680S. [Crossref]
16. NIH (2021) Folate -
Fact Sheet for Health Professionals. U.S. Department Health Human Services.
17. Allen LH, Peerson
JM, Olney DK (2009) Provision of multiple rather than two or fewer
micronutrients more effectively improves growth and other outcomes in
micronutrient-deficient children and adults. J Nutr 139: 1022-1030. [Crossref]
18. Muthayya S, Rah JH,
Sugimoto JD, Roos FF, Kraemer K et al. (2013) The global hidden hunger indices
and maps: an advocacy tool for action. PLoS One 8: e67860. [Crossref]
19. UNO (2016) Decade
of Action on Nutrition. United Nations Decade of Action on Nutrition.
20. Onyango A, Koski
KG, Tucker KL (1998) Food diversity versus breastfeeding choice in determining
anthropometric status in rural Kenyan toddlers. Int J Epidemiol 27:
484-489. [Crossref]
21. Baye K, Kennedy G
(2020) Estimates of dietary quality in infants and young children (6-23 mo):
Evidence from demographic and health surveys of 49 low- and middle-income
countries. Nutrition 78: 110875. [Crossref]
22. WHO. WHO Global
Nutrition Target: Stunting Policy Brief- What’s at stake.
23. Delgado CL (2003)
Rising consumption of meat and milk in developing countries has created a new
food revolution. J Nutr 133: 3907S-3910S. [Crossref]
24. FDA (2019) Dietary
Supplements. U.S. Food Drug Administration.
25. Bánhidy F, Ács N,
Puhó EH, Czeizel AE (2011) Iron deficiency anemia: pregnancy outcomes with or
without iron supplementation. Nutrition 27: 65-72. [Crossref]
26. WHO (2011)
Guideline : vitamin A supplementation in infants and children 6-59 months of
age. World Health Organization.
27. Islam MR, Attia J, Ali L, McEvoy M, Selim S et al. (2016)
Zinc supplementation for improving glucose handling in pre-diabetes: A double
blind randomized placebo controlled pilot study. Diabetes Res Clin Pract
115: 39-46. [Crossref]
28. WHO (2012)
Guideline: Daily Iron and Folic Acid Supplementation in Pregnant Women. Geneva:
World Health Organization. [Crossref]
29. Institute of
Medicine (US) Panel on Micronutrients (2001) Dietary Reference Intakes for
Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron,
Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc. Washington (DC):
National Academies Press (US). [Crossref]
30. Smith FR, Goodman
DS (1976) Vitamin A transport in human vitamin A toxicity. N Engl J Med
294: 805-808. [Crossref]
31. Ahmad A, Ahmed Z
(2019) Fortification in Beverages. Production and Management of Beverages
Volume 1: The Science of Beverages 85-122.
32. Mannar MGV, Wesley
AS (2008) Food Fortification. Int Encyclopedia Public Health 622-630.
33. Dobe M, Garg P,
Bhalla G (2018) Fortification as an effective strategy to bridge iron gaps
during complementary feeding. Clin Epidemiol Glob Heal 6: 168-171.
34. Dean JH, Pauly R,
Stevenson RE (2020) Neural Tube Defects and Associated Anomalies before and
after Folic Acid Fortification. J Pediatr 226: 186.e4-194.e4. [Crossref]
35. Dary O, Mora JO
(2013) Food Fortification: Technological Aspects. Encycl Human Nutr (Third
Edition) 306-314.
36. Hennessy Á, Walton
J, Flynn A (2013) The impact of voluntary food fortification on micronutrient
intakes and status in European countries: a review. Proc Nutr Soc 72:
433-440. [Crossref]
37. Tripathi B, Platel
K, Srinivasan K (2012) Double fortification of sorghum (Sorghum bicolor L.
Moench) and finger millet (Eleucine coracana L. Gaertn) flours with iron and
zinc. J Cereal Sci 55: 195-201.
38. McGee EJT,
Sangakkara AR, Diosady LL (2017) Double fortification of salt with folic acid
and iodine. J Food Eng 198: 72-80.
39. Modupe O, Diosady
LL (2021) Quadruple fortification of salt for the delivery of iron, iodine,
folic acid, and vitamin B 12 to vulnerable populations. J Food Eng 300:
110525. [Crossref]
40. Ramakrishnan U
(2002) Prevalence of micronutrient malnutrition worldwide. Nutr Rev 60:
S46-S52. [Crossref]
41. Akasapu K, Ojah N,
Gupta AK, Choudhury AJ, Mishra P (2020) An innovative approach for iron
fortification of rice using cold plasma. Food Res Int 136: 109599. [Crossref]
42. Tiozon RN Jr,
Camacho DH, Bonto AP, Oyong GG, Sreenivasulu N (2021) Efficient fortification
of folic acid in rice through ultrasonic treatment and absorption. Food Chem
335: 127629. [Crossref]
43. Bajaj SR, Singhal
RS (2021) Fortification of wheat flour and oil with vitamins B12 and D3: Effect
of processing and storage. J Food Compos Anal 96: 103703.
44. Rana B, Kaushik R,
Kaushal K, Arora S, Kaushal A et al. (2018)
Physicochemical and electrochemical properties of zinc fortified milk. Food
Biosci 21: 117-124.
45. Zahedirad M,
Asadzadeh S, Nikooyeh B, Neyestani TR, Khorshidian N et al. (2019) Fortification aspects of vitamin D in dairy products:
A review study. Int Dairy J 94: 53-64.
46. Bui LTT, Small DM
(2007) Folates in Asian noodles: II. A comparison of commercial samples and the
impact of cooking. J Food Sci 72: C283-C287. [Crossref]
47. Konar N, Poyrazoglu
ES, Artik N (2015) Influence of calcium fortification on physical and
rheological properties of sucrose-free prebiotic milk chocolates containing
inulin and maltitol. J Food Sci Technol 52: 2033-2042. [Crossref]
48. Tanumihardjo SA
(2018) Chapter 25 - Nutrient-Wise Review of Evidence and Safety of
Fortification: Vitamin A. Food Fortific Global World 247-253.
49. Mehra R, Srinivasan
K (2009) Chapter 75 - Iodine Fortification: Some Industrial Initiatives and
Concerns. Comprehensive Handbook Iodine 731-739.
50. Ohanenye IC,
Emenike CU, Mensi A, Medina Godoy S, Jin J et al. (2021) Food fortification technologies: Influence on
iron, zinc and vitamin A bioavailability and potential implications on
micronutrient deficiency in sub-Saharan Africa. Sci African 11: e00667.
51. Horton S, Wesley A,
Mannar MGV (2011) Double-fortified salt reduces anemia, benefit: cost ratio is
modestly favorable. Food Policy 36: 581-587.
52. Bouis HE, Hotz C,
McClafferty B, Meenakshi JV, Pfeiffer WH (2011) Biofortification: a new tool to
reduce micronutrient malnutrition. Food Nutr Bull 32: S31-S40. [Crossref]
53. Nestel P, Bouis HE,
Meenakshi JV, Pfeiffer W (2006) Biofortification of staple food crops. J
Nutr 136: 1064-1067. [Crossref]
54. Ekeleme V (2021)
Release of New Vitamin A Maize Varieties Sparks Optimism for Maize Farmers in
Nigeria. HarvestPlus Nigeria.
55. Laurie S, Faber M,
Adebola P, Belete A (2015) Biofortification of sweet potato for food and
nutrition security in South Africa. Food Res Int 76: 962-970.
56. Oke M, Seyoum
Workneh T (2013) A review on sweet potato postharvest processing and
preservation technology. Afr J Agric Res 8: 4990-5003
57. Mbogo D, Muzhingi
T, Janaswamy S (2021) Starch digestibility and β -carotene bioaccessibility in
the orange-fleshed sweet potato puree-wheat bread. 86: 901-906.
58. Finkelstein JL, Mehta S, Udipi SA, Ghugre PS, Luna
SV et al. (2015) A Randomized
Trial of Iron-Biofortified Pearl Millet in School Children in India. J Nutr
145: 1576-1581. [Crossref]
59. Haas JD, Luna SV,
Lung'aho MG, Wenger MJ, Murray Kol LE et
al. (2016) Consuming Iron Biofortified Beans Increases Iron Status in
Rwandan Women after 128 Days in a Randomized Controlled Feeding Trial. J
Nutr 145: 1586-1592. [Crossref]
60. Hull R, Head G,
Tzotzos GT (2021) Technologies for crop improvement. Genetically Modified
Plants 2021: 35-81.
61. Beyer P (2010)
Golden Rice and 'Golden' crops for human nutrition. N Biotechnol 27:
478-481. [Crossref]
62. Garcia Casal MN, Peña Rosas JP, Pachón H, De Regil LM, Tablante EC et al. (2016) Staple crops
biofortified with increased micronutrient content: effects on vitamin and
mineral status, as well as health and cognitive function in the general
population. Cochrane Database Syst Rev.
63. Fiedler JL, Kikulwe EM, Birol E (2013) An ex ante analysis of the impact and cost-effectiveness of biofortified high-provitamin A and high-iron banana in Uganda 44.
64. https://www.nal.usda.gov/sites/default/files/fnic_uploads/RDA_AI_vitamins_elements.pdf.