Management of Occult Spondylolisthesis in a Case of Low Back Pain
Management of Occult Spondylolisthesis in a Case of Low Back Pain
A B S T R A C T
Spondylolisthesis is a condition of the spine that causes lower back pain. It is a vertebra slippage that occurs at the base of the spine, in most instances. We report a case of occult spondylolisthesis of a patient with grade 1 spondylolisthesis (L4 over L5). We presented the radiologic finding, diagnosis, and treatment here. A 45-year-old female was presented with the complaints of low back pain with sciatica for 4 years. The radiologic finding showed that she had dysaesthesia on both L5 dermatome and MRI of LS Spine revealed prolapsed disc at L4/5. The patient underwent decompression, stabilization via pedicle screw at L4 and L5 with fusion at L4/5 and after constant follow-ups, she was symptom-free with a full range of motion of the spine. Posterior fusion with instrumentation of the pedicle screw is commonly considered the gold standard method of lumbar spinal fusion. Non-surgical treatment is effective in relieving low back pain of the patient in most cases however, symptomatic patients need to be treated with the surgical method.
Keywords
Spondylolisthesis, vertebra, dysaesthesia, low back pain
Introduction
Spondylolisthesis is the slippage of one vertebral body concerning the adjoining vertebral body causing mechanical or radicular side effects or agony. This "slip" as a rule happens when a locking instrument comprised by the laminae and facet joints has fizzled and may consequently stay static or progress after some time. It tends to be because of innate, gained, or idiopathic causes. Spondylolisthesis is evaluated by the level of slippage of one vertebral body on the adjoining vertebral body. Of cases, at the L4/L5 and L5/S1 levels, 90% happen [1]. Risk factors for spondylolisthesis incorporate a first-degree relative with spondylolisthesis, scoliosis, or mysterious spina bifida at the S1 level [2]. Clinically, lumbar spondylolisthesis might be asymptomatic or present with low back torment with or without alluded leg pain. Spondylolisthesis most ordinarily happens in the lower lumbar spine however can likewise happen in the cervical spine and infrequently, aside from injury, in the thoracic spine. Degenerative spondylolisthesis predominately happens in grown-ups and is more normal in females than males with expanded hazard in the obese.
Occult spondylolisthesis, with no undeniable plain radiographic highlights, can be appeared under unique stacking during MRI for back pain. Spondylolisthesis most generally happens at the L5-S1 level with the front interpretation of the L5 vertebral body on the S1 vertebral body. The L4-5 level is the second most regular area for spondylolisthesis. Grade I spondylolisthesis represents 75% of all things considered. Diagnosing the beginning phases of spondylolisthesis on plain radiography is difficult, in any event, when the slanted view is used [3, 4]. Several examinations have analysed MRI-recorded changes in dynamic spondylolisthesis, no investigations to date have decided the beginning recurrence of dynamic spondylolisthesis distinguished on MRI.
This study aims to report a case of occult spondylolisthesis and its appropriate treatment system in a patient with low back pain. Moreover, explicit clinical highlights of occult spondylolisthesis at the main clinical assessment were assessed to decide if they could help in early detection.
Case Report
A 45-year-old female was presented with the complaints of low backache with sciatica for 4 years. The pain increased on walking and relieved by taking rest. She was nondiabetic and normotensive. On examination there was a weakness in both extensors of the toes; SLR, Deep tendon reflexes were normal. She had dysaesthesia on both L5 dermatomes. MRI of LS Spine (Figure 1) revealed a prolapsed disc at L4/5. On dynamic X-ray, LS spine revealed grade 1 spondylolisthesis (L4 over L5) (Figures 2 & 3). The patient was subjected to decompression, stabilization at L4 and L5 by pedicle screw, with L4/5 fusion. The post-operative period was uneventful, and she was well recovered. Patient follow-up was conducted periodically. She was relieved of symptoms after 2 years of follow-up, with a complete range of spine motion.
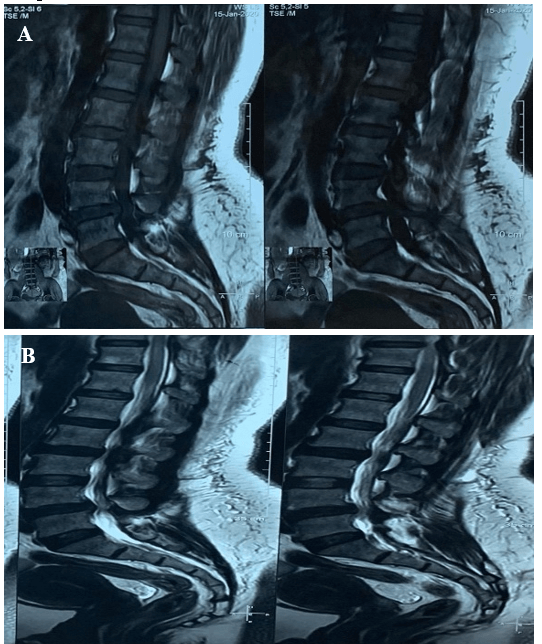
Figure 1: A) & B) MRI of Lumbosacral spine sagittal view showing disc bulge at L4/5 level.
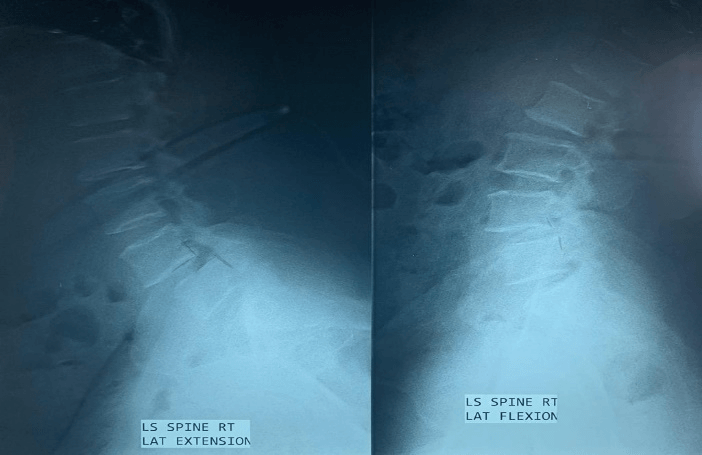
Figure 2: Functional X-ray Lumbosacral spine reveals L4/5 spondylolisthesis in Flexion view.
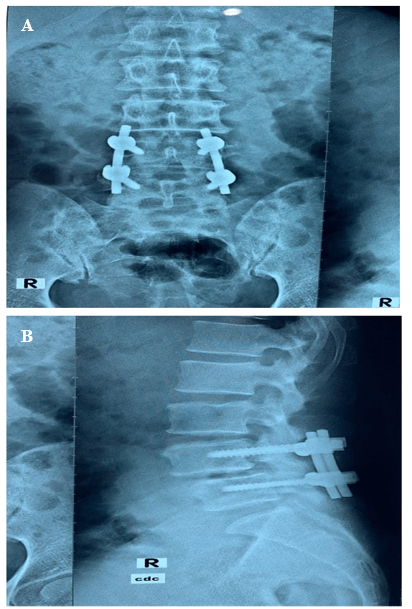
Figure 3: A) & B) Postoperative X-ray Lumbosacral spine showing transpedicular screw fixation with fusion at L4/5.
Discussion
The operative treatment of lumbar occult spondylolisthesis has always been controversial. The choices for surgical procedures include decompressive lumbar laminectomy and decompression with instrumented or non-instrumented transpedicular fusion [5-8]. The early identification and treatment of spondylolisthesis are related to improved healing and are significant for forestalling the movement of building pseudarthrosis [9-11]. Kalichman et al. announced no noteworthy relationship between spondylolisthesis, isthmic spondylolisthesis, or degenerative spondylolisthesis and the event of low back agony in their 3529 grown-up members on CT [12].
In the current study, the patient had a history of low back pain alongside sciatica and dysaesthesia on both L5 dermatomes. Maurer et al. reported that of the 22 asymptomatic juvenile rowers in their study, 5 demonstrated the high signal intensity of the pars interarticularis on T2-weighted MRI scans, and none showed manifestations related with spinal issues as long as 3 months after the end of the study [13]. For this current study, MRI of LS Spine revealed a prolapsed disc at L4/5. On dynamic X-ray, LS spine revealed grade 1 spondylolisthesis (L4 over L5). The MRI permitted the identification of dynamic degenerative spondylolisthesis, consistent with the clinical picture. Utilizing MRI, we had the option to show that the marvel of instability in spondylolisthesis does happen and that pathologic highlights may show more plainly under stacking. This finding may suggest it as a radiographic help with continuing with surgical decompression.
The unsteadiness of spondylolisthesis is generally debated. Past studies have demonstrated a relationship between the level of slip and disc height reduction in adults, potentially brought about by degeneration incited segmental ligamentous laxity [14]. An examination by Iguchi et al. proposed that translational changes had more suggestive results than angulation and pressure [15]. Instability and the dynamic idea of degenerative spondylolisthesis can be appeared by standard radiography alone, yet open MRI procedures to observe the intersegmental versatility of the lumbar spine with spondylolisthesis have been studied previously [16].
It this study, the patient went through decompression, adjustment using pedicle screw at L4 and L5 with the combination at L4/5. It is recommended that even decompression may prompt the destabilization of the motion segment. In later studies, it has been demonstrated that instrumented combination brings about an improved and expanded fusion rate after posterolateral fusion for degenerative spondylolisthesis, even though there are no critical contrasts in clinical results regarding pain and daily life activities [17, 18]. Our study findings are intriguing and propose that it should be considered a conceivably helpful system in patients with clinical manifestations and indications of neurogenic claudication that might be caused by spondylolisthesis, which is occult on plain radiography or traditional MRI.
Conclusion
The surgical management of occult spondylolisthesis is a considerable challenge at present. After long-term follow-up, the patient presented in this study recovered post-operatively and demonstrated a symptom free better life. Hence it can be concluded that even in such cases, decompression, and stabilization via pedicle screw with fusion surgery will result in favourable outcomes with a high patient satisfaction rate. For whatever reason, symptomatic patients need to be treated by conservative or surgical options. The skilled hands represent an effective treatment and are commonly correlated with good clinical and neurological performance.
Article Info
Article Type
Case ReportPublication history
Received: Mon 31, Aug 2020Accepted: Thu 10, Sep 2020
Published: Thu 24, Sep 2020
Copyright
© 2023 Md. Moshiur Rahman. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.09.19
Figures & Tables
References
- Newman PH, Stone KH (1963) The etiology of spondylolisthesis. J Bone Joint Surg Br 45-B: 39-59.
- Rachel M Randall, Michael Silverstein, Ryan Goodwin (2016) Review of Pediatric Spondylolysis and Spondylolisthesis. Sports Med Arthrosc Rev 24: 184-187. [Crossref]
- C J Harvey, J L Richenberg, A Saifuddin, R L Wolman (1998) The radiological investigation of lumbar spondylolysis. Clin Radiol 53: 723- 728. [Crossref]
- N Papanicolaou, R H Wilkinson, J B Emans, S Treves, L J Micheli (1985) Bone scintigraphy and radiography in young athletes with low back pain. AJR Am J Roentgenol 145: 1039-1044. [Crossref]
- A J Caputy, A J Luessenhop (1992) Long-term evaluation of decompressive surgery for degenerative lumbar stenosis. J Neurosurg 77: 669-676. [Crossref]
- J Cauchoix, M Benoist, V Chassaing (1976) Degenerative spondylolisthesis. Clin Orthop Relat Res 115: 122-129. [Crossref]
- H N Herkowitz, L T Kurz (1991) Degenerative lumbar spondylolisthesis with spinal stenosis. A prospective study comparing decompression with decompression and intertransverse process arthrodesis. J Bone Joint Surg Am 73: 802-808. [Crossref]
- T A Zdeblick (1993) A prospective, randomized study of lumbar fusion. Preliminary results. Spine 18: 983-991. [Crossref]
- K Fujii, S Katoh, K Sairyo, T Ikata, N Yasui (2004) Union of defects in the pars interarticularis of the lumbar spine in children and adolescents: the radiological outcome after conservative treatment. J Bone Joint Surg Br 86: 225-231. [Crossref]
- Antonio Leone, Alessandro Cianfoni, Alfonso Cerase, Nicola Magarelli, Lorenzo Bonomo (2011) Lumbar spondylolysis: a review. Skeletal Radiol 40: 683-700. [Crossref]
- Koichi Sairyo, Shinsuke Katoh, Yoichiro Takata, Tomoya Terai, Natsuo Yasui et al. (2006) MRI signal changes of the pedicle as an indicator for early diagnosis of spondylolysis in children and adolescents: a clinical and biomechanical study. Spine 31: 206-211. [Crossref]
- Leonid Kalichman, David H Kim, Ling Li, Ali Guermazi, Valery Berkin et al. (2009) Spondylolysis and spondylolisthesis: prevalence and association with low back pain in the adult community-based population. Spine 34: 199-205. [Crossref]
- Marvin Maurer, Ricardo Bernardi Soder, Matteo Baldisserotto (2011) Spine abnormalities depicted by magnetic resonance imaging in adolescent rowers. Am J Sports Med 39: 392-397. [Crossref]
- B E Fredrickson, D Baker, W J McHolick, H A Yuan, J P Lubicky (1984) The natural history of spondylolysis and spondylolisthesis. J Bone Joint Surg Am 66: 699-707. [Crossref]
- Tetsuhiro Iguchi, Aritetsu Kanemura, Koichi Kasahara, Keizo Sato, Akira Kurihara et al. (2004) Lumbar instability and clinical symptoms: Which is the more critical factor for symptoms: Sagittal translation or segment angulation? J Spinal Disord Tech 4: 284-290. [Crossref]
- R D Bellah, D A Summerville, S T Treves, L J Micheli (1991) Low-back pain in adolescent athletes: detection of stress injury to the pars interarticularis with SPECT. Radiology 180: 509-512. [Crossref]
- K H Bridwell, T A Sedgewick, M F O'Brien, L G Lenke, C Baldus (1993) The role of fusion and instrumentation in the treatment of degenerative spondylolisthesis with spinal stenosis. J Spinal Disord 6: 461-472. [Crossref]
- J S Fischgrund, M Mackay, H N Herkowitz, R Brower, D M Montgomery et al. (1997) 1997 Volvo Award winner in clinical studies. Degenerative lumbar spondylolisthesis with spinal stenosis: A prospective, randomized study comparing decompressive laminectomy and arthrodesis with and without spinal instrumentation. Spine 22: 2807-2812. [Crossref]