Local Swelling and Redness Associated with Supraclavicular Nerve Injury
A B S T R A C T
Supraclavicular nerves are at risk in operative procedures when surgical incisions are placed over the clavicle. This report describes a 50-year-old man who developed local swelling and redness of the supraclavicular region after undergoing Weaver-Dunn reconstruction of the coracoclavicular ligament. ENMG was consistent with supraclavicular nerve injury. Since the symptoms may mimic infection, the awareness of this complication will aid the clinician to avoid unnecessary use of antimicrobials.
Keywords
Clavicular fracture, nerve injury, electroneuromyography, supraclavicular nerve, coracoclavicular ligament
Introduction
Supraclavicular nerves sustain an iatrogenic injury in operative procedures when a surgical incision is placed in the clavicular region [1]. Peripheral nerve injuries are associated with reactive changes of the skin [2]. Peripheral nerve injury may result in sympathectomy leading to vasodilatation in the affected area, which causes redness and swelling. Supraclavicular nerve is particularly vulnerable to injury during procedures of the clavicle, and numbness is common after surgery of the clavicle or acromioclavicular joint [3]. This case presents illustrative photos of a patient with reactive hyperemia due to supraclavicular nerve injury [1].
Case Report
A 50-year-old male underwent Weaver-Dunn reconstruction of the left coracoclavicular ligament from a sagittal skin incision. Immediately after the procedure the skin on the lateral side of the wound was numb. The skin incision healed normally. Local redness and swelling developed during the weeks following the procedure laterally from the sagittal skin incision. Figure 1A shows the left shoulder 2 weeks after the procedure. The area with lack of sensation corresponded to the segment innervated by the lateral supraclavicular nerve (marked with black stripes in Figure 1B). Electroneuromyography was consistent with an iatrogenic complete laceration of the lateral supraclavicular nerve.
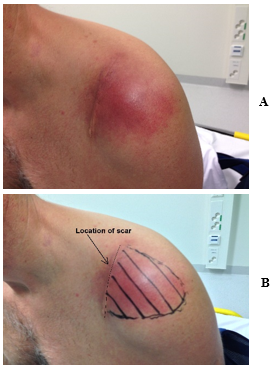
Figure 1: A) Local hyperemia of the left shoulder after a Weaver-Dunn procedure performed from a sagittal incision. B) The area of numbness and the location of the scar are drawn. Unlike with infection, the hyperemia is located unilaterally on the distal side of the scar.
Discussion
I would hypothesize that a cutaneous sympathectomy was the cause of transient local skin hyperemia that resolved spontaneously during the following month. Surgeons should be aware of this complication, as the clinical manifestation may be mistaken for infection and lead to unnecessary antibiotic treatments. Supraclavicular nerve injuries are not uncommon after surgery of the clavicular region, but nerve entrapment may also occur after a clavicular fracture [1, 3, 4]. The resulting post-operative numbness form nerve injury may result in patient dissatisfaction [3]. Surgeons should be aware of safe zones or use meticulous dissection when performing surgery close to supraclavicular nerves [5].
Funding
None.
Conflicts of Interest
None.
Consent
Consent was obtained from the patient.
Article Info
Article Type
Case ReportPublication history
Received: Tue 01, Jun 2021Accepted: Sat 11, Sep 2021
Published: Wed 29, Sep 2021
Copyright
© 2023 Markus Pääkkönen. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.09.07
Figures & Tables
References
1.
Mehta
A, Birch R (1997) Supraclavicular nerve injury: the neglected nerve? Injury
28: 491-492. [Crossref]
2.
Kurvers
HA, Jacobs MJ, Beuk RJ, Van den Wildenberg FA, Kitslaar PJ et al. (1995) Reflex
sympathetic dystrophy: evolution of microcirculatory disturbances in time. Pain
60: 333-340. [Crossref]
3.
O´Neill
K, Stutz C, Duvernay M, Schoenecker J (2012) Supraclavicular nerve entrapment
and clavicular fracture. J Orthop Trauma 26: e63-e65. [Crossref]
4. Wang K, Dowrick A, Choi J, Rahim R, Edwards E (2010) Post-operative numbness and patient satisfaction following plate fixation of clavicular fractures. Injury 41: 1002-1005. [Crossref]
5. Nathe T, Tseng S, Yoo B (2011) The anatomy of the supraclavicular nerve during surgical approach to the clavicular shaft. Clin Orthop Relat Res 469: 890-894. [Crossref]