Let's "Twist it": Retrieval of a Guidewire Fragment in Complex Coronary Angioplasty – Case Report
A B S T R A C T
Percutaneous transluminal coronary angioplasty is a useful management strategy in the treatment of ischemic heart disease, nevertheless, complex percutaneous coronary interventions could result in device fracture or dislodgement. We report and discuss a case of successful retrieval of fractured guide wire from a bypass graft - native vessel anastomosis using the twisting wire technique.
Keywords
Guide wire fracture, retrieval of lost device, twisting wire technique
Introduction
Percutaneous transluminal coronary angioplasty (PTCA) is a useful management strategy in the treatment of ischemic heart disease, nevertheless, in increasingly complex percutaneous coronary interventions, the risk of device fracture or dislodgement should be taken into account, even if, such occurrences are infrequent they may pose an unfamiliar and challenging problem for the treating interventional cardiologist [1]. The management of such complications is challenging and can be resolved by conservative management, percutaneous retrieval method, or eventually surgically [2, 3]. We report a case where the extraction of a fractured angioplasty guidewire using three standard 0.014-inch angioplasty guidewires. This case highlights the hazards of deploying stents in small, calcific, distal e tortuous graft vessel and the management of removal of the fractured guidewire in coronary intervention.
Case Report
A 74-year old male with a history of dyslipidemia, hypertension diabetes with severe renal and peripheral comorbidity, with a background of known severe coronary artery disease. The patient had undergone coronary artery bypass grafting in 2004 with a right internal mammary artery graft to the left anterior descending artery, left internal mammary artery graft to the obtuse marginal, and saphenous vein bypass grafts to the distal right coronary artery and the diagonal artery. In 2018 the patient complained typical angina and underwent a coronary angiogram that demonstrated diffusely severe disease of the native coronaries and occlusions of the saphenous vein bypass grafts; the internal mammary arteries were severely calcified and diseased however resulted patent. After an unsuccessful attempt of PTCA of the saphenous vein bypass grafts to the diagonal artery, he underwent a reducer insertion in order to treat his chronic angina symptoms. The patient was free of symptoms until 2019, where he presented with chest discomfort with the initial evidence of left ventricular failure.
The electrocardiogram demonstrated a diffuse ST depression and known complete right bundle block; troponin measurements were significantly abnormal. Due to the diagnosis of the acute coronary syndrome non-ST myocardial infarction, the patient proceeded to coronary angiography. Diagnostic catheterization performed from the right radial artery demonstrated similar coronary condition except for a significant progression of the disease resulting in obstructive of the anastomosis of right internal mammary artery graft to the left anterior descending artery, and its distal tract (Figure 1). The patient proceeded to a percutaneous coronary intervention of the anastomosis of the right internal mammary artery graft and the left anterior descending artery.
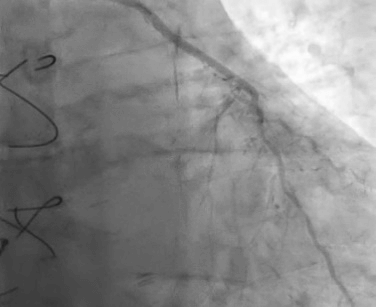
Figures 1: Coronary angiography before angioplasty.
We have engaged the right internal mammary artery graft with a 6F IMA™ guide catheter (Medtronic - Minneapolis, MI, USA) using a right radial approach as the femoral approach was not possible for significant vessel disease. Intra-arterial heparin was administered at the start and during the procedure to achieve a constant activated clotting time of more than 250 seconds; we did not administer any glycoprotein IIb/IIIa inhibitors as the patient was already on long term antiplatelet therapy.
For the significant vessel tortuosity and the lack of backup support, in order support the guide in a coaxial position for optimal device delivery we firstly proceeded with an anchoring technique using a Balance Middleweight (BMW) 0.014-inch guidewire (Guidant Corp., Indianapolis, Indiana, U.S.A) and a 2.0 x 12mm Maverick™ Balloon (Boston Scientific crop., Natick, Massachusetts, U.S.A) inserted in a collateral vessel resulting in successful coaxial catheter position; therefore, facilitating the vessel wiring (Figure 2), afterwards in order to achieve further support due to the severity of vessel tortuosity a Hi-Torque Versaturn™ and a Hi-Torque BMW Universal™ 0.014 inch guidewires (Abbott Vascular, Abbott Park, IL, U.S.A) were introduced into the distal tract of the left anterior descending artery and in the diagonal branch, due to the highly calcified vessel we firstly proceeded with lesion predilataion using small diameter balloons of 1.0 x 10 mm Sapphire™ NC Balloon (OrbusNeich, Hoevelaken, Netherland), 1.25 x 15 mm Tazuna™ Balloon (Terumo Medical Corporation; Somerset, NJ, U.S.A) and finally with a 2.0 x 15 mm Maverick™ Balloon (Boston Scientific) and then stented on the anastomosis and middle vessel tract with two Xience Sierra™ (Abbott), 2.5 x 23 mm and distally to it in partial overlap with another Xience Sierra™ (Abbott) 2.25 x 28 mm stent. Final stents dilatation was obtained with a 2.5 x 15 mm and 3.0 x 15 mm Emerge™ Balloons (Boston Scientific) with an excellent result in the main vessel.

Figures 2: Anchoring technique before vessel wiring.
During attempts to retract the BMW Universal™ guidewire (Abbott Vascular) positioned in the main vessel, it became apparent that the distal radio-opaque portion of the wire was fixed in the distal coronary artery tract resulting in subsequent unraveling and fracture of the guidewire (Figure 3).
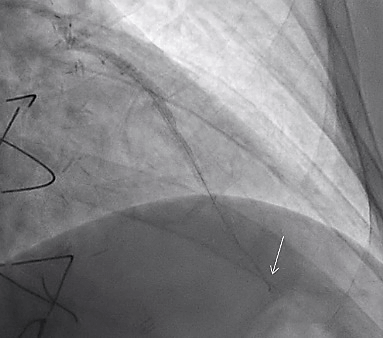
Figures 3: Distal radio-opaque portion of the wire fracture (arrow).
Retrieval Technique
A triple wire technique was chosen in order to retrieve the distal wire. In essence, adequate wire entanglement with 3 BMW 0.014-inch guidewire (Guidant Corp) were sequentially introduced in the proximal tract of the RIMA; all three wires were inserted into the torque device (Abbott Vascular) and then rotated together further to entangle the proximal fractured segment (Figure 4). The entangled collection was then carefully extracted. Final angiography confirmed no wire residua noted with a good result of PTCA (Figure 5): Overall procedural time was 120 minutes with 170cc contrast liquid of VISIPAQUE™ (GE Healthcare Inc., Marlborough, Massachusetts, U.S.A), Fluoroscopic time was 59 minutes. The patient resulted asymptomatic for chest pain or dyspnea at the end of the procedure and dismissed after a few days. Three months later, the patient underwent a coronary control angiogram that demonstrated a good result of the previous PTCA; we did not proceed with further coronary angioplasty of the distal tract of the left anterior descending artery.
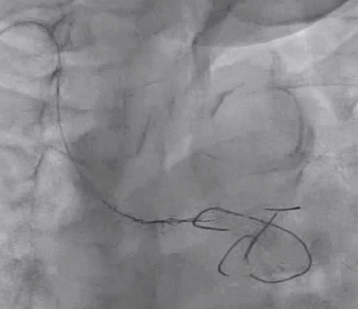
Figures 4: Three guidewires entangle twisting technique.
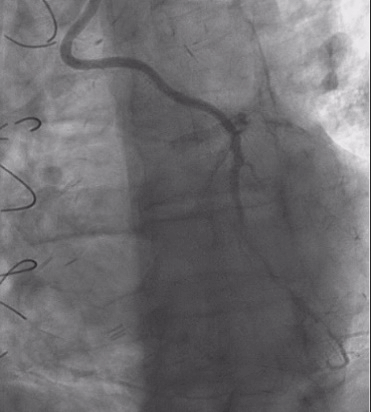
Figures 5: Final angiography.
Discussion
We describe a case that for our best knowledge is the first to describe a successful coronary guidewire twisting technique in a graft vessel with the interest of anastomosis tract of a native severely diseased and calcified left anterior descending artery, resulting in full recovery of the patient and without any need of major surgery or significant renal impairment, even if the technique is not retained novel, the overall complicity and procedure risks of such procedure in presented patient is not considered to be acknowledged as usual daily practice; in fact, results obtained from PubMed website including keywords “coronary intervention” and “twisting wire technique” resulted poorly, therefore suggesting therefore, moderate utilization and experience of such technique preferring other solutions, or somewhat poorly reporting for abscess of interest for the lack of “challenge” in an overall low infrequent complication, either is mainly retained as a bailout technique in cases of device dislocation, or finally a technique to could be held as a novel method during coronary thrombus aspiration procedure [3, 4].
PTCA procedure risks in patients with graft and coronary vessels with a high burden of calcification and atherosclerosis should be particularly taken into account, not only during stent positioning but however also with further importance in case of guidewire fracture; therefore, it is challenging and should be considered in complex long time procedures involving hydrophilic guidewires in calcified and tortuous vessels. Management options depend upon the extent of the retained material, the clinical status of the patient, and the size, relevance, and characteristics of the involved vessel, moreover, awareness of the different options for device extraction and operator experience and skills are essential. Several solutions have been proposed; such as leaving the guidewire, adding, therefore, an anticoagulant to already onboard dual antiplatelet therapy resulting therefore in higher bleeding risk, moreover, includes the extraction of the dislodged with a snare; however, such a device is more suitable for proximal, large-caliber vessels and requires periodically expertise, therefore, could result in further complications such as migration in other major arteries [5].
Other invasive options could include inflation of a balloon in order to trap the fractured guidewire however in the retrieval of such debris in a distal tract of a bypass graft could lead not only to endothelial damage to the vessel due to the retraction of the guidewire but also in alteration of the stent(s) architecture. Stenting over the retained guidewire in order to crush it could be useful if the vessel diameter is appropriate; however, it would result not only in further consumption of devices but also in longer and more complicated intervention and possible clinical consequences. Finally, an open-heart surgery could be taken into account in order to remove the fragment; however, it should be taken into account the operational risks in a patient with dual antiplatelet therapy onboard or with previous CABG procedure [6].
Finalizing, in our case, the main vessel wire might have impinged upon one of the two stent struts in a heavily calcific vessel; thus, we have decided for a simple solution of device extraction using three simple guidewires.
Conclusion
The complicated coronary procedure includes risks of fracture or dislodgement of equipment. Where various solutions such as conservative, aggressive invasive, or surgery options are valid possibilities, our solution of using three angioplasty guidewires to entangle the fractured guidewire resulted in being a useful and straightforward method in the management and problem resolution.
Highlights
• Percutaneous transluminal coronary angioplasty is a useful management strategy in the treatment of ischemic heart disease.
• The risk of device fracture or dislodgement should be taken into account, especially in coronary angioplasty of complex lesions.
• We describe a case of extraction of a fractured angioplasty guidewire due to a complication during a complex coronary angioplasty of a bypass-native vessel anastomosis.
Article Info
Article Type
Case ReportPublication history
Received: Mon 27, Apr 2020Accepted: Mon 11, May 2020
Published: Wed 20, May 2020
Copyright
© 2023 Alon Schaffer. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.05.08
Figures & Tables
References
- Iturbe JM, Abdel-Karim AR, Papayannis A, Mahmood A, Rangan BV et al. (2012) Frequency, treatment, and consequences of device loss and entrapment in contemporary percutaneous coronary interventions. J Invasive Cardiol 24: 215-221. [Crossref]
- Ahmad T, Chithiraichelvan S, Patil TA, Jawali V (2016) Surgical retrieval of entrapped coronary angioplasty guidewire from the aorta. Asian Cardiovasc Thorac Ann 24: 81-84. [Crossref]
- Feldman T (1999) Retrieval techniques for dislodged stents. Catheter Cardiovasc Interv 47: 325-326. [Crossref]
- Zou YL, Li JQ, Gong YT, Sun DH, Li Y (2020) A novel treatment of refractory coronary embolism: thrombus aspiration catheter-assisted twisting wire technique. J Geriatr Cardiol 17: 110-115. [Crossref]
- Abe D, Sato A, Misaki M, Takeyasu N, Aonuma K (2014) Miraculous catch of a broken coronary guidewire tip in the right internal carotid artery. Int J Cardiol 176: e1-e2. [Crossref]
- Al-Moghairi AM, Al-Amri HS (2013) Management of retained intervention guide-wire: a literature review. Curr Cardiol Rev 9: 260-266. [Crossref]