Leptomeningeal Cyst in the Adult: Case Report and Review of the Literature
A B S T R A C T
Background: Leptomeningeal cysts are a rare complication of childhood fractures, being very rare in adulthood and usually related to previous trauma generated in children.
Case Presentation: We present a case of “growing fracture” in a 70-year-old woman with a history of head injury in childhood, who clinically debuted with paresthesia-dysesthesia in the left hemicranium and hypersensitivity and pain in the affected area, and who was treated with surgical treatment.
Conclusion: We review the pathogenesis, diagnosis and treatment of this injury today.
Keywords
Leptomeningeal cyst, growing fracture, skull fracture, adult, dural defect, cranioplastic
Background
The leptomeningeal cyst, also known as “growing fracture”, is a rare complication of skull fractures with an incidence below 1% that occurs predominantly in the pediatric population, especially in children under 3 years of age. Its incidence in adulthood contains few references in the literature and is usually related to previous trauma generated in pediatric age [1-10]. A clinical case of a leptomeningeal cyst is presented in a 70-year-old woman with a history of head trauma.
Case Presentation
A 70-year-old woman with a history of severe head trauma at age 7 was under study by Neurology in relation to cephalo-paresthesia and probable nummular headache. The patient reported paresthesia-dysesthesia in the left hemicranium of several years of evolution and hypersensitivity and pain in the affected area. On examination, she only presented pain at the tip of her left parietal finger, with no other neurological focus. The cranial computed tomography (CT) showed a left parietal deformity of probable post-traumatic origin with an underlying extra-axial cystic formation of approximately 3 x 2.1 cm that remodels the internal table, suggesting associated expansiveness (Figure 1).
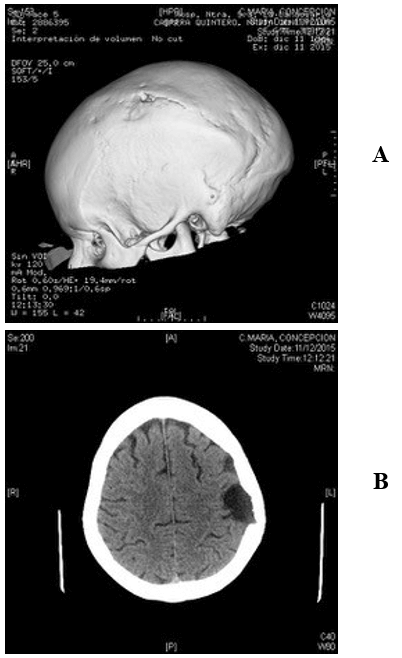
Figure 1: A & B) The cranial CT showed a left parietal deformity of probable post-traumatic origin with an underlying extra-axial cystic formation of approximately 3 x 2.1 cm that remodels the internal table, suggesting expansiveness.
The magnetic resonance imaging (MRI) described a 34 x 22 mm cystic lesion in the left frontoparietal region, with altered signal in the parenchymal margin of the lesion and an expansive effect both towards the parenchyma and towards the internal table, conditioning its remodeling, associated with discontinuity of the shell and a lesion with similar intradiploic characteristics of about 12 x 5 mm. These findings were compatible with a leptomeningeal cyst (“growing fracture”) (Figure 2).
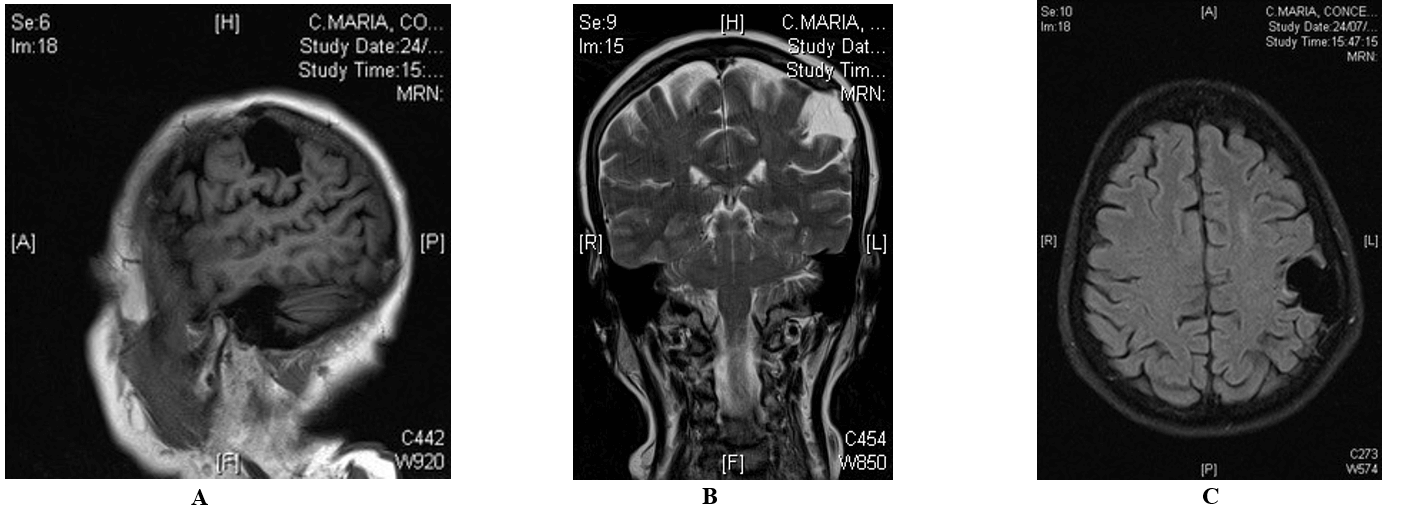
Figure 2: A, B & C) The brain MRI shows a cystic lesion in the left frontoparietal region with an expansive effect both towards the parenchyma and towards the internal table, conditioning its remodeling, associated with discontinuity of the calvaria and a lesion with similar intradiploic characteristics of about 12 x 5 mm.
A wide craniotomy was performed around the visible margins of the lesion, observing cerebrospinal fluid leakage with significant erosion of the associated internal cortex and the leptomeningeal cyst in depth. Reconstruction of the dural defect with suturable dura was performed, and we opted to replace the autologous cranioplasty associated with acrylic cement. In the postoperative period, the patient presented motor dysphasia that evolved favourably.
Discussion
Leptomeningeal cysts are characterized by progressive growth of the fracture, with an increase in dehiscence at the edges of the same, which can lead to deformities [8]. The first description of the growth of the skull after the fracture was made by Howship in 1816, and the term leptomeningeal cyst was introduced by Dyke in 1937 [2, 6, 8, 10, 11]. Another term used today is evolutionary fracture [11]. The incidence of progressive fractures is 0.5-1% in the series reviewed, especially in the pediatric population, being more frequent in children under 3 years of age. Presentation in adulthood is rare, with very few cases published after review [1-10].
The most frequent location in all age groups is in the parietal region, but there are cases described in other cranial areas such as the orbital roof and posterior fossa, both locations present in adults [5, 6, 11, 12]. The pathogenesis of these lesions is still controversial, but for most authors, there must be a dural defect underlying a previous fracture and a mechanical force that causes the herniation of the leptomeningeal through the defect, and that may be due to edema, contusion, hydrocephalus, or the heartbeat itself [6, 8, 13]. The most frequent origin of the fracture is the presence of previous head trauma, although iatrogenic cases have also been published. In general, they are detected early in the first year of the trauma, but in the adult population, they can manifest late, even after 10 years [4].
Lende and Erickson describe four determining factors for the diagnosis of leptomeningeal cyst: i) skull fracture in childhood, ii) tear of dura mater, iii) underlying brain injury, and iv) growth of the fracture [2, 8, 10]. There are three types of evolutionary fracture described by Rahman et al.: Type I) the herniation of arachnoid tissue without modification of the ventricular system, Type II) the appearance of encephalocele and the ventricle grows towards the fracture, Type III) the existence of the porencephalic cavity that communicates with the ventricular system [8]. From a diagnostic point of view, a physical examination is essential, observing a soft, non-pulsatile mass on the scalp [8]. In the pediatric population, the presence of pain or headache is rare, being more common in the adult population [10]. The most frequent symptom in the adult population is seizures [6].
The imaging tests used in the diagnosis are radiography, cranial CT and brain MRI [3, 14]. Radiography shows a fracture whose edges are separated in relation to the previous radiography, these being irregular, spiculated or everted. CT is the diagnostic test of choice, allowing us to see edge dehiscence, the existence of an associated brain injury, or deformity of the ventricular system. MRI is very useful to identify associated lesions clearly and for differential diagnosis, including arachnoid cyst and epidermoid cyst [8, 12].
The recommended treatment for leptomeningeal cysts is surgery using a combined dura-cranioplasty technique (autologous or alloplastic) to expose and reconstruct the underlying defect [3, 7, 8, 10-12, 15].
Conclusion
The leptomeningeal cyst in adults is an atypical situation little described in the literature that can be detected up to more than 10 years after the head injury. They are usually parietal in location, with surgical treatment being the one performed in most cases.
Acknowledgement
None.
Availability of Data and Materials
All data supporting the conclusions of this article are included within the published article.
Funding
None.
Ethical Approval and Consent to Participate
Not applicable.
Abbreviations
CT: Computed Tomography
MRI: Magnetic Resonance Imaging
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing Interests
None.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Mon 11, Jan 2021Accepted: Tue 26, Jan 2021
Published: Mon 08, Feb 2021
Copyright
© 2023 Paula Pilar Morales Cejas. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.02.05
Figures & Tables
References
- Yan XH, Qiu K, Gao Y, Ren J, Cheng D et al. (2020) Growing Skull Fracture of Temporal Bone in Adults: A Case Report and Literature Review. Ear Nose Throat J 99: 654-657. [Crossref]
- Kale A, Aydogmus E, Açikgöz B (2016) Clinically Adult Onset of a Leptomeningeal Cyst After Head Trauma in Childhood: Case Report and Review of the literatura. Neurosurg Q 26.
- Kim H, Jo KW (2013) Treatment of a Traumatic leptomeningeal Cyst in an Adult with frinogen- based collagen. J Korean Neurosurg Soc 53: 300-302. [Crossref]
- Saito A, Sugawara T, Akamatsu Y, Mikawa S, Seki H (2009) Adult traumatic leptomeningeal cyst: case report. Neurol Med Chir (Tokyo) 49: 62-65. [Crossref]
- Meier JD, Dublin AB, Strong EB (2009) Leptomeningeal Cyst of the Orbital Roof in an Adult: case report and literaure review. Skull Base 19: 231-235. [Crossref]
- Houra K, Beros V, Sajko T, Cupic H (2006) Traumatic Leptomeningeal Cysts in a 24-year-old man: Case Report. Neurosurgery 58: E201. [Crossref]
- Kurosu A, Fujii T, Ono G (2004) Post-Traumatic leptomeningeal cyst mimicking a skull tumour in adult. Br J Neurosurg 18: 62-64. [Crossref]
- González MJ, Cutrín Prieto JM, García Pravos A, Muñuzuri AP, Fernández Villa JM (2000) Quiste leptomeníngeo postraumático de larga evolución. Neurocirugía 11: 224-230.
- Kutlay M, Demircam N, Akin ON, Basekim C (1998) Untreated growing cranial fractures detected in late stage. Neurosurgery 43: 72-76. [Crossref]
- Britz GW, Kim DK, Mayberg MR (1998) Traumatic Leptomeningeal cyst in an adult: A case report and review of the literatura. Surg Neurol 50: 465-469. [Crossref]
- Muhonen MG, Piper JG, Menezes AH (1995) Pathogenesis and treatment of growing skull fractures. Surg Neurol 43: 367-373. [Crossref]
- Seo BR, Lee JK, Jeong IH, Moon SJ, Joo SP et al. (2009) Post- traumatic intradiploic leptomeningeal cyst of the posterior fossa in an adult. Cases Reports. J Clin Neurosci 16: 1367-1369. [Crossref]
- Singh V, Shetty GS, Naik S, Behari S, Phadke RV (2016) Intradiploic Leptomeningeal cyst in an adult: role of percutaneous contrast injection in dural defect demostration. Acta Neurochir (Wien) 158: 301-304. [Crossref]
- Onizuka K, Momma F, Ohara S, Ohyama T (1994) Emerging symtoms of growing skull fracture after secondary trauma in an adult--case report. Neurol Med Chir (Tokyo) 34: 807-809. [Crossref]
- Açiköz B, Tekkök IH (2002) Post-traumatic intradiploic leptomeningeal fistula and cyst. J Clin Neurosci 9: 468-73. [Crossref]