Laparoscopic Approach for Esophagojejunal Anastomotic Leak in Patients Requiring Re-Look Intervention: How We Do It
A B S T R A C T
Background: Esophagojejunal anastomotic leak (EJAL) is a serious and often a life-threatening complication following total gastrectomy. There is no standard management strategy, and the optimal approach remains controversial. Whilst non-operative approach (with or without percutaneous drainage), endoscopic approach (stents, clips, and vacuum devices) is the preferred initial management, and there remains a subset of EJAL patients that require operative intervention because of the uncontrolled leak with sepsis and potential high mortality.
Methods: We present early clinical results of a minimally invasive novel surgical technique (continuous suction isoperistaltic jejuno-esophagostomy tube, SIJET) to divert saliva and enteric secretions away from the anastomotic area thus creating a hypothesised concept of “no leak” scenario. The details of this technique are described and illustrated.
Results: This is the first clinical report of a laparoscopic technique for insertion of SIJET in two patients with esophagojejunal anastomotic leaks managed successfully. Both patients had failed to progress on non-operative management because of the uncontrolled leak with sepsis.
Conclusion: The absolute prerequisite for complete healing of an anastomotic leak is adequate drainage of undrained fluid collections and diversion of luminal fluid away from the anastomotic defect. Laparoscopic SIJET provides a minimally invasive option for the management of esophagojejunal leak following total gastrectomy in patients with uncontrolled leak with sepsis.
Keywords
Laparoscopic surgery, total gastrectomy, esophagojejunal leak, isoperistaltic tube suction
Introduction
Esophagojejunal anastomotic leak following total gastrectomy is associated with significant morbidity and mortality [1-5]. Optimal management remains controversial, whether non-operative, endoscopic therapy, or re-operation [3]. Depending on the patient’s clinical condition, non-operative (conservative) management has its advocates but may lead to delayed intervention with increase morbidity and mortality [1, 3]. Endoscopic therapy including the use of stents, clips or Endovac methods has been used with variable success, requiring further investigation [1, 3]. Re-operation particularly in the form of laparotomy and ‘re-do’ anastomosis carries the highest risk of morbidity and mortality of around 60% [1-4]. However, when non-operative or endoscopic approaches failed in the setting of on-going leak and sepsis, the only feasible option is re-look intervention. In these technical notes, we emphasize a prompt return to the operating room after computerized tomography (CT)-contrast imaging of chest and abdomen to detect undrained collections and uncontrolled leak. We then proceed to a laparoscopic approach with washout for peritonitis and drainage of any collection followed by placement of a continuous suction isoperistaltic jejuno-esophagostomy tube (SIJET).
Methods
Surgical Technique
I Equipment
1 x Jagwire™ (Boston Scientific) (0.035in x 260cm); 1 x 18F nasogastric tube (NGT); 1 x 28F intercostal catheter (ICC); 1 x jejunostomy feeding tube (if not already established).
II Steps for Laparoscopic Placement of SIJET (Figure 1)
i. Laparoscopic approach to the esophagojejunal anastomotic area in conjunction with simultaneous endoscopy to assess the location and extent of the leak. If the defect can be seen and accessible laparoscopically, close the defect with 3-0 monofilament sutures Otherwise if the defect is in a posterior location or the anastomosis is high in the mediastinum, it should be left intact.
ii. Check the length of the alimentary limb of the Roux-en-Y reconstruction; establish the most proximal point of this limb, which can reach the anterior abdominal wall, usually about 25cm from the anastomosis. Mark this point with a laparoscopic marking pen.
iii. The gastroscope is advanced to the marked point via the anastomosis. The stiff end of a 260cm JagwireTM inserted through the scope then traverse the jejunal wall and pull out through the left upper quadrant port. The gastroscope is now removed while firmly holding on the JagwireTM outside the laparoscopic port. A small jejunostomy is created at the JagwireTM site (Figure 1).
iv. A 18F NGT with a cut tip is advanced orally over the JagwireTM (Seldinger technique) to the left upper quadrant port. A 28F ICC is then advanced retrogradely over the NGT through the same 12mm laparoscopic port into the jejunum. The tube is then advanced into the esophagus to 10cm above the anastomosis, with position confirmed on endoscopy. The NGT and JagwireTM can then be removed.
v. Jejunostomy site is purse-stringed around the ICC with a 3-0 V-LOC suture (Covidien, Mansfield MA) and then attached to the peritoneal surface of the anterior abdominal wall with 3-0 PDSTM (Figure 2).
vi. SIJET arrangement is then secured to the skin with 0-0 silk suture.
vii. Feeding jejunostomy is established for enteral nutrition. A Jackson-PrattTM drain is placed adjacent to the anastomotic site.
viii. SIJET is connected to 25cm of water on wall suction on return to the ward.
The patient should be kept nil by mouth. Intravenous fluids and electrolytes for maintenance and losses as well as antibiotics are administered accordingly. Jejunostomy tube feeds may be started as soon as possible or when ileus is resolved. Around postoperative day 6 or 7, oral methylene-blue dye test followed by GastrografinTM swallow to assess anastomotic integrity with the SIJET clamped. Once confirmed, oral clear fluids and puree diet upgraded thereafter. The SIJET can then be removed after 4 weeks.
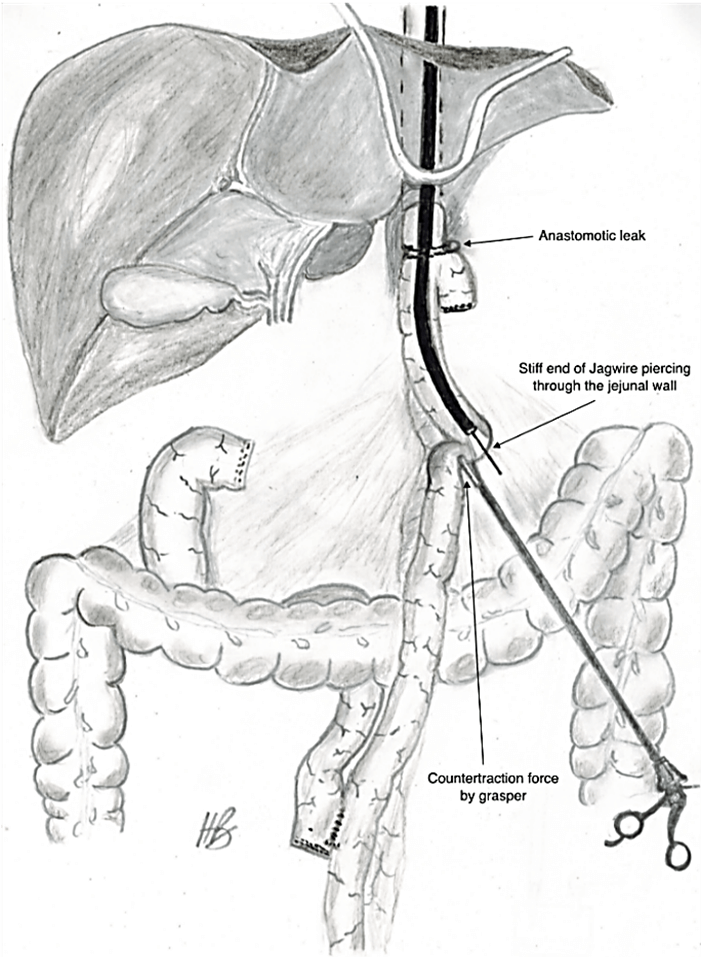
Figure 1: Jagwire inserted through gastroscope then through the jejunal wall and out through the left upper quadrant laparoscopic port.
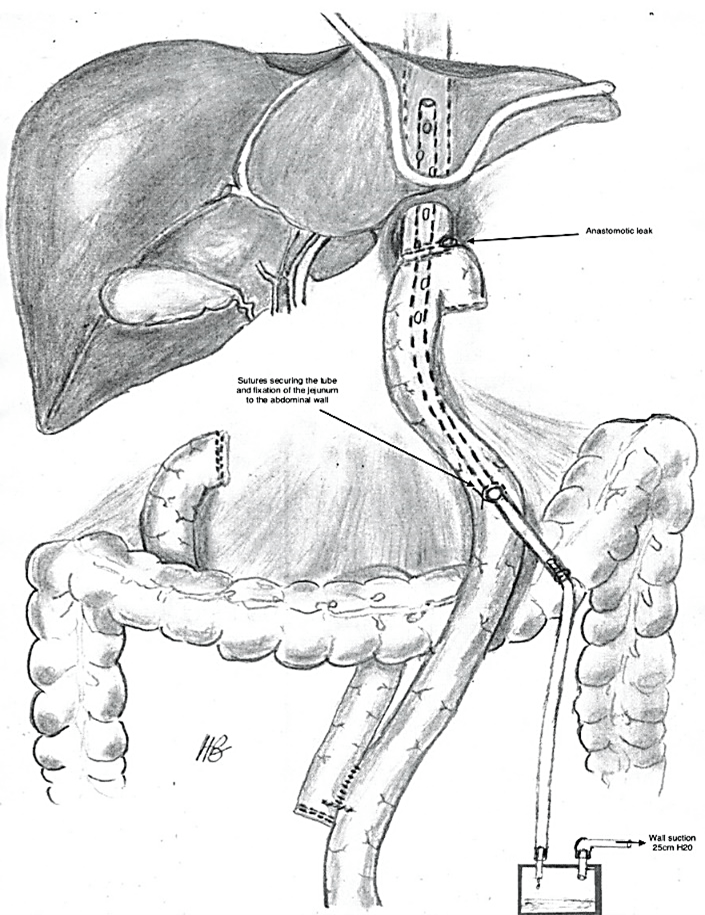
Figure 2: Suction isoperistaltic jejuno-esophagostomy tube above the anastomotic leak and connected to continuous wall suction.
Results
The laparoscopic procedure for placement of SIJET was performed safely in two patients. Both patients had undergone total gastrectomy for cancer and developed postoperative EJAL. Initial non-operative management including large-bore nasojejunal tube suction and supportive care failed to improve the clinical situation with on-going evidence of sepsis and uncontrolled leak. Following laparoscopic SIJET, the average time to full oral diet was 22 days for the two patients. No leaks or skin excoriation were encountered at the SIJET exit sites and all wounds were completely healed at 2 weeks after SIJET removal.
Discussion
SIJET allows diversion of both saliva and enteric secretions and through creating a negative intraluminal pressure secondary to continuous suction, relieves tension around the anastomotic site. Additionally, the SIJET provides local control of a septic focus and reduce the potential for peritoneal and mediastinal soiling. As leak is a dynamic process, if all air, saliva, and enteric secretions are diverted away through SIJET, there should be no leak by definition. Along with sepsis control and nutritional support, SIJET provides a favourable environment for healing by secondary intention. These principles are akin to those used in the EndoVac method which require multiple trips to the operating theatres for replacing the EndoVac under general anaesthesia [6].
Prevailing literature on the outcomes of esophagojejunal leaks, highlighted that late detection and difficult “re-do” anastomosis were factors associated with the highest risk of morbidity and mortality [1, 2, 4]. Our emphasis on early detection in the setting of uncontrolled leak and sepsis and minimally invasive approach for the two cases of esophagojejunal leaks with success further endorse the principles of continuous isoperistaltic tube suction for management of leaks in upper gastrointestinal surgery. Applying the same principles of SIJET, but with continuous suction isoperistaltic gastro-esophagostomy tube (SIGET), we have managed three cases of lower esophageal perforations and two cases of proximal gastric pouch leak post-Roux-en-Y gastric bypass after unsuccessful lap-band treatment [7].
Conclusion
For the subset of patients that require ‘re-look’ intervention for esophagojejunal leak because of the uncontrolled leak with sepsis, laparoscopic SIJET provides a minimally invasive additional management option. We would strongly advocate the principles of SIJET be applied even if an open approach is adopted.
Author Contributions
Both H T Bui and S T F Chan contributed equally to the study design, data collection, data analysis, writing and revision of this manuscript.
Funding
None.
Conflicts of Interest
None.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Article Info
Article Type
Research ArticlePublication history
Received: Thu 04, Feb 2021Accepted: Thu 18, Feb 2021
Published: Tue 09, Mar 2021
Copyright
© 2023 Steven T F Chan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.03.01
Figures & Tables
References
1. Makuuchi R, Irino T, Tanizawa Y, Bando E, Kawamura T et al. (2019) Esophagojejunal anastomotic leakage following gastrectomy for gastric cancer. Surgery Today 49: 187-196. [Crossref]
2. Sierzega M, Kolodziejczyk P, Kulik J Polish Gastric Cancer Study Group (2010) Impact of anastomotic leakage on long-term survival after total gastrectomy for carcinoma of the stomach. Br J Surg 97: 1035-1042. [Crossref]
3. Carboni F, Valle M, Federici O, Sandri GBL, Camperchioli I et al. (2016) Esophagojejunal anastomosis leakage after total gastrectomy for esophagogastric junction adenocarcinoma: options of treatment. J Gastrointest Oncol 7: 515-522. [Crossref]
4. Aurello P, Magistri P, D’Angelo F, Valabrega S, Sirimarco D et al. (2015) Treatment of esophagojejunal anastomosis leakage: a systematic review from the last two decades. Am Surg 81: 450-453. [Crossref]
5. Gong W, Li J (2017) Combat with esophagojejunal anastomotic leakage after total gastrectomy for gastric cancer: A critical review of the literature. Int J Surg 47: 18-24. [Crossref]
6. Kuehn F, Schiffmann L, Janisch F, Schwandner F, Alsfasser G et al. (2016) Surgical endoscopic vacuum therapy for defects of the upper gastrointestinal tract. J Gastrointest Surg 20: 237-243. [Crossref]
7. Vu AN, Bui HT, Abulrasool H, Chan STF (2019) Continuous Suction Isoperistaltic Gastroesophagostomy for Esophageal Perforation. Ann Thorac Surg 107: e293-e295. [Crossref]