Intravesical Explosion Resulting in Bladder Rupture During Transurethral Resection of Prostate: A Case Report
A B S T R A C T
Transurethral resection of prostate (TURP) is one of the most common surgeries in urology. Intravesical explosion during transurethral resection is an extremely rare event. It usually leads to bladder rupture, which can be either extra-or intra-peritoneal requiring urgent laparotomy. We report a case of intravesical blast in a 70-year-old male undergoing TURP.
Keywords
Bladder rupture, intravesical explosion, transurethral resection
Introduction
Transurethral resection of prostate (TURP) forms one of the main surgical and endoscopic approach towards removal of the inner portion (primarily the transition zone) of the prostate that encircles the urethra [1]. The monopolar TURP requires the use of a nonionic irrigant (water, glycine, sorbitol) to allow electro resection of the prostate [1]. Most patients undergoing monopolar TURP (M-TURP) have an uneventful intraoperative and postoperative course. M-TURP has been associated with a considerable intraoperative complication rate in spite of its use clinically since decades. Although the overall complication rate has improved, there is still at least a 3% chance of intraoperative complications, primarily hemorrhage leading to transfusion [2].
Intravesical blast or explosion during transurethral surgery is a very rare complication of transurethral resection of prostate or transurethral resection of bladder tumors [3]. It usually leads to bladder rupture, which can be either extra- or intra-peritoneal requiring urgent laparotomy. It occurs due to the generation and trapping of explosive gases under the dome of the bladder. Although this complication is rare, but the morbidity associated with this complication is high. We report a case of intravesical blast in a 70-year-old male undergoing M-TURP.
Case Report
A 70-year-old patient was admitted to Urological services of the hospital with symptomatic benign enlargement of the prostate. Patient was on alpha blockers (Silodosin 8 mg od) since a year and patient had no relief of symptoms. Serum prostate specific antigen was 4.17 ng/mL. A transrectal guided biopsy of the prostate revealed benign pathology. Patient was advised monopolar TURP for relief of symptoms.
Under regional anaesthesia (spinal) the patient was positioned and TURP done. The resected chips were washed out and the resectoscope reintroduced to observe the fossa. During the inspection a few bleeders were coagulated. During this procedure there was a loud sound from within the bladder and the bladder collapsed around the scope. Irrigation was not returning; hence a diagnosis of bladder perforation was made, and the patient explored using an infra-umbilical midline incision. The bladder was ruptured irregularly like that of a blast or explosion injury (Figure 1). The torn margins were identified, and the bladder closed in two layers using 00 vicryl suture. A supra-pubic catheter was also left in place. Post-operatively the patient had an uneventful recovery. The drain was removed after 72 hours, supra-pubic catheter removed after a week and the periurethral catheter removed after 2 weeks. The patient voided well after catheter removal with no residual urine.
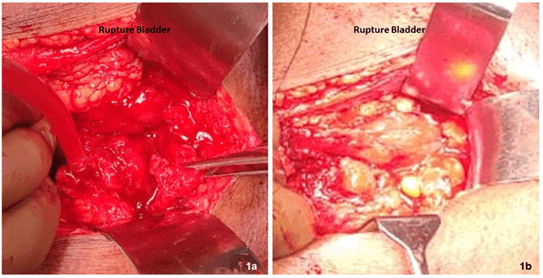
Figure 1: a) Shows ruptured anterior bladder wall with large defect. b) Bladder after repair.
Discussion
Intravesical explosion or blast is an extremely rare event associated with transurethral resection of the prostate. Bladder injury can range from mucosa tear to bladder rupture. Such explosions have also been described when using diathermy during colonic surgery and large bowel endoscopies [4]. Mild explosions in the bladder generally do not cause complications, however, severe explosions may result in significant morbidity, including mortality in elderly patients.
The trapping of volatile gases during resection of tissue is the mechanism for the bladder explosion. These volatile gases are an admixture of hydrogen and explosive hydrocarbons [4]. Several authors have demonstrated both in vitro and in vivo that hydrogen (30~65%) was the dominant gas produced during transurethral resection of prostate (TURP), oxygen and several explosive hydrocarbons were produced in small amounts [3]. Majority of these gases are produced from pyrolysis of human tissues and electrolysis of intracellular water due to high temperatures associated with cutting and coagulation of tissues. When hydrogen gets mixed with oxygen from the atmosphere, it becomes inflammable and gets ignited by a spark generated by electrosurgery [4]. The amount of gas formed, and the risk of explosion are proportional to the temperature of the resectoscope and operating time [4].
Lower abdominal tenderness, bleeding from the bladder and a restless patient are the usual symptoms of such an occurrence. These patients need to be explored immediately and the bladder repaired. Patients may need blood transfusions and admission to critical care wards.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Case ReportPublication history
Received: Wed 17, Feb 2021Accepted: Tue 06, Apr 2021
Published: Mon 26, Apr 2021
Copyright
© 2023 R. B. Nerli . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.03.13
Figures & Tables
References
1. Welliver C, McVary KT Minimally Invasive and Endoscopic Management of Benign Prostatic Hyperplasia. In Campbell.
2. Ahyai SA, Gilling P, Kaplan SA, Kuntz RM, Madersbacher S et al. (2010) Meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic enlargement. Eur Urol 58: 384-397. [Crossref]
3. Pathak A, Singh M, Ramappa A, Jain S, Rasool S et al. (2018) Intravesical explosion during transurethral resection of prostate: Prevention and management. Urol Ann 10: 111-113. [Crossref]
4. Lee CC, Chang HK, Chen M, Hsu JM (2014) Intravesical Explosion Resulting in Bladder Rupture During Transurethral Resection of Bladder Tumors. Int J Gerontol 8: 230-231.