Hypospadias in Twins
A B S T R A C T
Hypospadias is one of the most common birth defects among male children. Many associated risks for hypospadias have been reported like family history, older maternal age, nulliparity, high pre-pregnancy body mass index of mother, hypertension or preeclampsia, multiple gestations, low birth weight, and small for gestational age. In literature twinning as a risk factor has been consistently shown to be associated with hypospadias. We report a 2-year-old male child (one of the twins) who presented with proximal microphallic hypospadias.
Keywords
Twins, hypospadias, birth defect, risk factors
Introduction
Hypospadias is a common congenital disorder wherein the external urethral opening lies proximal to the normal glanular location [1, 2]. This defect is considered to be due to arrested development although embryos do not exhibit a similar appearing phase [3]. Hypospadias is known to occur 1 in every 300 males (0.3%). The risk of occurrence is nearly 13 times greater in first-degree relatives (brothers, fathers, offspring) [3]. Several studies have also reported regarding familial clustering of hypospadias with ≈ 7% of the patients reporting hypospadias in first- or second-degree relatives [4, 5]. As reported by Brouwers et al., low birth weight, being a twin or triplet, fertility treatments, mother being a diethylstilbestrol-daughter, paternal subfertility, obesity, prescriptive drug use, and familial occurrence of hypospadias were associated with increased risk of hypospadias in general [6]. Low birth weight (a proxy for placenta dysfunction) seemed much strongly associated with proximal hypospadias with an OR (95%CI) of 9.1 (3.4-24.2) as compared with distal and middle hypospadias at 2.6 (1.4-5.0) and 2.3 (0.8-6.5). We report a 2-year-old male child who presented with proximal microphallic hypospadias and has a twin brother who was operated at 9 months’ age for perimembranous ventricular septal defect (L to R) with severe pulmonary arterial hypertension and sinus rhythm.
Case Report
A 2-year-old male child presented to the pediatric urological services with a small sized hypospadiac penis. He was one of the monochorionic twins (antenatal scans). The other twin was diagnosed to have perimembranous ventricular septal defect (L to R) associated with severe pulmonary arterial hypertension and sinus rhythm and underwent Sauvage patch closure of VSD at the age of 9 months. There was no history of consanguity and the twins were born at full term. No history of use drugs during pregnancy, assisted reproduction or, exposure to pesticides during pregnancy.
On examination the child was conscious and playful. The penis appeared microphallic with proximal penile hypospadias and chordee (Figure 1). The stretched penile length was 18mm and the diameter of glans was 11 mm. The testes were fully descended bilaterally, and no other obvious anomalies were seen. The parents were counselled regarding the starting of preoperative hormonal treatment with injection testosterone 2mg/Kg body weight once a month, for three months. The penile length and girth increased following injections and the parents were counselled for surgical repair of the hypospadias.
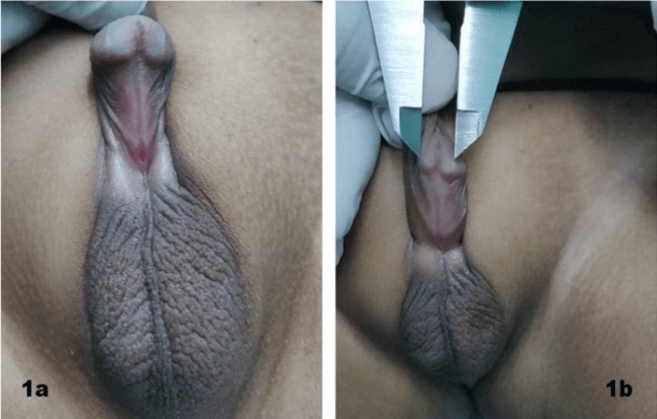
Figure 1: a & b) Proximal penile hypospadias.
Discussion
There has been an increase in the rate of twins worldwide, probably because of assisted [5]. The rate of twin births in USA increased by 75% from ~ 18.9 to 33.2 twins per 1000 births) [7]. The reason for this increase has been attributed to increasing use of fertility treatments. It is well established that twins in comparison with singletons are at increased risk for several adverse outcomes including low birth weight, preterm birth and infant mortality [8]. Among the twins the monozygotic (MZ) twins are at an increased risk of birth defects compared to both singletons and dizygotic (DZ) twins [9].
The aetiology of isolated hypospadias is mainly multifactorial, and several factors such as genetic, endocrine, environmental, and clinical factors have all been observed. Twinning is a consistent risk factor that has been found to associated with hypospadias [10, 11]. Rider et al. reported that hypospadias occurred more often in twins compared with singletons (adjusted odds ratio (OR) 2.1 (95% CI: 1.5- 3.1) [9]. In birth weight discordant twins, hypospadias is more frequently observed in the twin with the lowest birth weight [12]. When genetic factors get ruled out in monozygotic twin pairs, Environmental etiological risk factors appear to be important. Visser et al. reported the incidence of hypospadias in monochorionic group was 4% (14/350) and dichorionic groups was 1% (3/303) (p= 0.016) respectively. In 11 of the 15 twin couples, hypospadias occurred in the twin with the lowest birth weight. The rate of hypospadias in twin infants small-for-gestational- age group was high (10%) as compared with 2% in the appropriate-for-gestational-age group (p=0.002). In a multivariate analysis the independently associated factors with hypospadias were monochorionicity and small-for-gestational-age.
It is also well known that hypospadias occurs more frequently in small for gestation age (SGA) infants [13]. This association between SGA and hypospadias suggests that there could be an association between placental insufficiency and abnormal genital development. Nutrients and gonadotropins would become inadequate for the normal development of the two pairs of male gonads in twin pregnancies due to inadequate placentation or unequal placental sharing [14, 15]. The smaller twin would be more sensitive to relative deficit in hormones, hence at an increased risk of developing hypospadias. Monochorionic twins have an increased risk for hypospadias. Monochorionic and SGA were identified to be independently associated with hypospadias.
Funding
None.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Wed 17, Feb 2021Accepted: Wed 07, Apr 2021
Published: Wed 05, May 2021
Copyright
© 2023 R. B. Nerli . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.03.14
Figures & Tables
References
1.
Nerli RB, Guntaka
AK, Patil RA, Patne PB (2014) Dorsal inlay inner preputial graft for primary
hypospadias repair. Afr J Paediat Surg 11: 105-108. [Crossref]
2.
Visser R, Burger
NC, van Zwet EW, Hilhorst Hofstee Y, Haak MC et al. (2015) Higher incidence of
hypospadias in monochorionic twins. Twin Res Hum Genet 18: 591-594. [Crossref]
3.
Campbell SC, Lane
BR et al. (2016) Malignant renal tumors. Campbell-Walsh Urol.
4.
Fredell L,
Iselius L, Collins A, Hansson E, Holmner S et al. (2002) Complex segregation
analysis of hypospadias. Hum Genet 111: 231-234. [Crossref]
5.
Nerli RB, Ghagane
SC, Neelgund SE, Hiremath MB, Dixit NS (2018) Familial Aggregation of
Hypospadias in South Indian Population. Res J Congenit Dis 1: 1-4.
6.
Brouwers MM, van
der Zanden LF, De Gier RP, Barten EJ, Zielhuis GA et al. (2010) Hypospadias:
risk factor patterns and different phenotypes. BJU Int 105: 254-262. [Crossref]
7.
Martin JA,
Hamilton BE, Ventura SJ, Osterman MJ, Mathews TJ (2013) Births: final data for
2011. Natl Vital Stat Rep 62: 1-69. [Crossref]
8.
Chauhan SP,
Scardo JA, Hayes E, Abuhamad AZ, Berghella V (2010) Twins: prevalence,
problems, and preterm births. Am J Obstet Gynecol 203: 305-315. [Crossref]
9.
Rider RA,
Stevenson DA, Rinsky JE, Feldkamp ML (2013) Association of twinning and
maternal age with major structural birth defects in Utah, 1999 to 2008. Birth
Defects Res A Clin Mol Teratol 97: 554-563. [Crossref]
10. Brouwers MM, Feitz WF, Roelofs LA, Kiemeney LA, De
Gier R et al. (2007) Risk factors for hypospadias. Eur J Pediatr 166:
671-678. [Crossref]
11. Nordenvall AS, Frisén L, Nordenström A, Lichtenstein
P, Nordenskjöld A (2014) Population based nationwide study of hypospadias in
Sweden, 1973 to 2009: incidence and risk factors. J Urol 191: 783-789. [Crossref]
12. Chambers CD, Castilla EE, Orioli I, Jones KL (2006)
Intrauterine growth restriction in like‐sex twins discordant for structural
defects. Birth Defects Res A Clin Mol Teratol 76: 246-248. [Crossref]
13. Fredell L, Lichtenstein P, Pedersen NL, Svensson J,
Nordenskjold A (1998) Hypospadias is related to birth weight in discordant
monozygotic twins. J Urol 160: 2197-2199. [Crossref]
14. Nerli R, Bindu S, Guntaka AK, Patil SM, Neelgund SE et
al. (2010) Maternal risk factors associated with hypospadias. Recent Res Sci
Technol 2: 30-34.
15. Hussain N, Chaghtai A, Herndon CA, Herson VC,
Rosenkrantz TS et al. (2002) Hypospadias and early gestation growth restriction
in infants. Pediatrics 109: 473-478. [Crossref]