Endoluminal Vacuum Therapy for Esophageal Anastomotic Leakage Following Multivisceral Transplantation: A Case Report
A B S T R A C T
Background: Esophageal anastomotic leakage is a rare but potentially life-threatening complication, especially following complex surgical procedures like multivisceral transplantation. Endoluminal negative pressure therapy (ENPT) has emerged as a promising, minimally invasive strategy to treat gastrointestinal anastomotic leakage outside the setting of immunosuppression. However, its application in transplant recipients has not been described yet. Case Presentation: We report the case of a 47-year-old woman who underwent multivisceral transplantation due to diffuse splanchnic ischemia, secondary to celiac trunk and superior mesenteric artery thrombosis. Postoperatively, she developed persistent epigastric pain and respiratory distress, prompting ICU readmission. A CT-scan and upper endoscopy revealed an anastomotic leakage at the level of the esophago-gastric anastomosis. Given her clinical condition, ENPT therapy was chosen after multidisciplinary discussion. A VACStent® prosthesis was positioned endoscopically. Three ENPT sessions resulted in complete resolution of the anastomotic leakage, which was confirmed on contrast gastrografin swallow radioscopy. Conclusion: Our case illustrates the potential of ENPT in immunocompromised high-risk patients. Consequently, it may be considered a safe and effective alternative to surgical or prosthetic interventions, emphasizing the expanding role of advanced endoscopic therapies in complex postoperative scenarios.
Keywords
Endoluminal negative pressure therapy, esophageal anastomotic leakage, gastrointestinal perforation, immunosuppression, multivisceral transplantation, splanchnic ischemia, VACStent®
Introduction
Multivisceral transplantation is a complex, life-saving procedure indicated for patients suffering from diffuse abdominal disease not treatable by any other means, typically diffuse splanchnic venous or arterial thrombosis, tumours and combined liver and intestinal failure [1, 2]. Despite significant advances in surgical techniques and immunosuppressive protocols, postoperative complications remain frequent and challenging to manage [3, 4, 5].
Esophageal anastomotic leakage, although rare, is a clinically significant event associated with high morbidity and mortality if not promptly recognized and treated [6]. When preventive measures [7] fail, management options include surgical repair, stent placement, or more recently, advanced endoscopic techniques [8]. Among these, endoluminal negative pressure therapy (ENPT) has gained popularity in managing gastrointestinal leakage in the setting of esophageal resection, due to its local conditions improving properties and limited invasiveness [9].
Multivisceral transplantation entails an anastomosis between the native esophagus and the transplanted stomach. Here, we report a rare case of esophageal suture leakage in a patient following multivisceral transplantation.
Case Presentation
A 47-year-old woman underwent multivisceral transplantation due to diffuse splanchnic ischemia, secondary to simultaneous thrombosis of the celiac trunk (CT) and the superior mesenteric artery (SMA). The abdominal organs (liver, stomach, duodeno-pancreas, small intestine) were procured en-bloc from a 14-year-old female brain-dead donor.
Pre-operative selective embolization of the inferior mesenteric artery (AMI) was performed [4, 10]. Following resection of the gastro-intestinal bloc (stomach, duodeno-pancreas, intestine, spleen), an aortic conduit (AC) was constructed from the donor’s thoracic aorta and anastomosed to the recipient’s infrarenal aorta. After hepatectomy, graft implantation began with caval replacement, followed by anastomosis of the aortic patch (containing donor CT and SMA) to the AC. An esophago(recipient)-gastric(donor) anastomosis was constructed. The patient was supported intraoperatively with continuous veno-venous hemofiltration and veno-venous bypass. Perioperatively, shortly after graft reperfusion, the patient experienced a brief episode of cardiac arrest due to hyperkalemia-induced ventricular fibrillation. Due to cardiac arrest, a second look at 24h post-transplant was planned, where we completed the esophago-gastric anastomosis by a Toupet fundoplication and a pylorotomy. Abdominal closure was done by non-vascularized rectus fascia transplant and standard skin closure with ileostoma construction (Figure 1) [11].
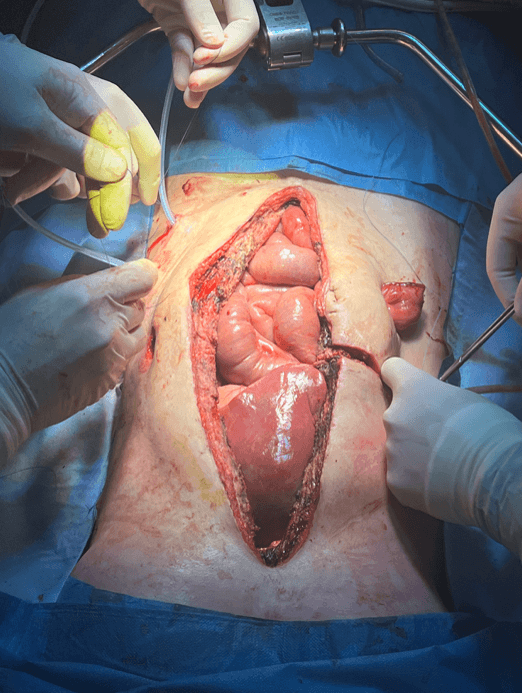
Figure 1: Perioperative images showing abdominal closure with creation of an ileostomy.
The patient was transferred to the intensive care unit (ICU) for postoperative monitoring. Empiric antibiotic therapy with piperacillin-tazobactam was initiated. However, intraoperative cultures of peritoneal fluids later grew Escherichia coli - resistant to tazobactam – and Enterococcus faecium. Antibiotics were adjusted to meropenem and vancomycin accordingly.
The nasogastric tube was removed on post operative day (POD) 12, and oral intake with pudding was restarted cautiously. Due to poor appetite, oral intake remained insufficient, and enteral nutrition via jejunostomy was initiated to meet caloric requirements.
On POD 17, inflammatory markers showed a mild increase, although the patient remained clinically stable. A contrast-enhanced CT-scan of the thorax and abdomen showed no evidence of bleeding or expanding collections. Given her stable condition, the patient was transferred to the regular ward on POD 20.
On POD 22, she developed persistent epigastric pain, respiratory discomfort, and a mild rise in inflammatory markers. An urgent non-contrast thoracoabdominal CT-scan with peroral contrast revealed a suspicious image for anastomotic leakage at the level of the esophago-gastric anastomosis, prompting her return to the ICU. The anastomotic leakage was confirmed by upper endoscopy (Figure 2A). Considering the patient's overall condition and the location of the defect, a conservative approach was selected. Endoluminal negative pressure therapy (ENPT) was initiated with placement of an EsoSponge®. ENPT was initiated within 24 hours after radiological suspicion and immediate endoscopic confirmation of the defect, aiming to achieve early source control and prevent further septic deterioration. Two chest drains were placed and empirical antifungal therapy with caspofungin was added to the antimicrobial therapy.
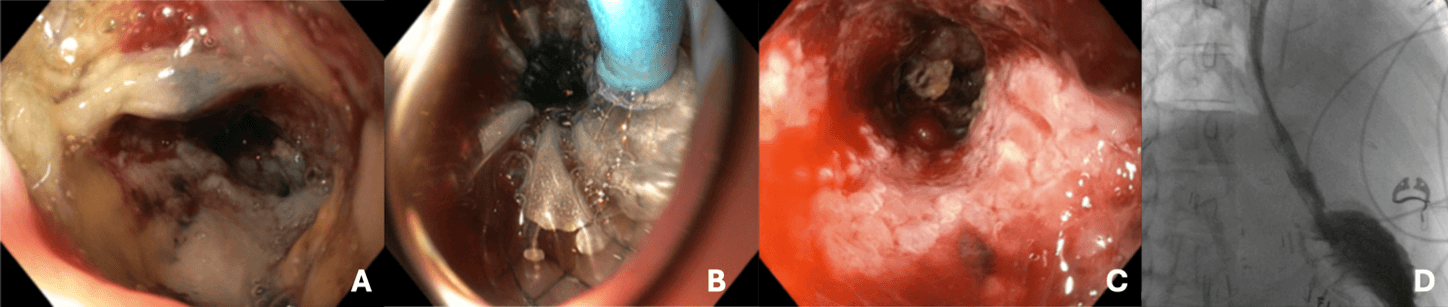
Figure 2: Endoscopic view of: A) esophageal leakage. B) VACStent®: The prosthesis was deployed in the esophagus over a guidewire and measured 7 cm in length, a 14 mm body diameter, and a 30 mm calyx diameter. C) Healed esophagus. D) Follow-up contrast swallow radioscopy on POD 38: the post-treatment contrast study demonstrates good transit of contrast medium across the esophago-gastric anastomosis, without any radiological signs suggestive of anastomotic dehiscence or contrast leakage.
On POD 25, the EsoSponge® was replaced; however, the defect had enlarged and was no longer suitable for sponge therapy. After multidisciplinary discussion involving thoracic surgeons, transplant surgeons, gastroenterologists, and intensivists, it was decided to opt for a VACStent®. The decision was based on the progressive enlargement of the defect, insufficient sealing with sponge therapy alone, and the need to combine defect coverage with continuous negative pressure therapy while minimizing surgical morbidity in this immunocompromised patient. The prosthesis was deployed in the esophagus over a guidewire and measured 7 cm in length, a 14 mm body diameter, and a 30 mm calyx diameter (Figure 2B).
On POD 27, a CT scan revealed slight enlargement of a left hypochondrial collection, raising suspicion of superinfection. A percutaneous drain was placed, and E. faecium was cultured from the fluid.
According to our VACStent® ENPT protocol, endoscopic reassessment was performed every 5–7 days. The first VACStent® exchange was carried out after 6 days, followed by a second exchange after another 5 days. Each session included cavity inspection, irrigation, and repositioning of the device to maintain effective negative pressure therapy until complete resolution of the defect.
Three ENPT sessions were performed and demonstrated a gradual reduction in the size of the cavity, ultimately leading to a complete resolution (Figure 2C). On POD 37, the VACStent® was removed, and a nasogastric tube was left in place. A gastrografin swallow radioscopy performed on POD 38 demonstrated no evidence of leakage (Figure 2D). The patient resumed oral intake by POD 40 and was transferred back to a regular room by POD 51.
Despite this resolution, her infectious state persisted, and pleural fluid analysis confirmed the presence of limited grade I-II empyema with E. faecium, secondary to the esophageal leak. A left-sided pigtail drain was placed, and antibiotic therapy was continued, resulting in gradual resolution of the infection.
On POD 45, a follow-up gastrografin swallow radioscopy confirmed the absence of leakage. The nasogastric tube was removed, and oral feeding was gradually resumed.
Follow-up endoscopy revealed progressive stricture at the esophago-gastric anastomosis, for which she received a series of graded balloon dilations on a weekly basis. However, because of recurring stenosis between the dilatation sessions, a radial incision of the fibrotic anastomosis, using electrocauterization, was performed. Since then, no further dilatations or other interventions were required and oral intake was continued.
At 6-month follow-up, the patient remained clinically stable, with adequate oral intake, no radiological evidence of recurrent leakage, and stable graft function under standard immunosuppressive therapy.
Discussion
Esophageal anastomotic leakage is a rare but potentially life-threatening complication, particularly in the context of multivisceral transplantation in which also requires an an aortic tube anastomosis. Therefore, the aorta is at risk for developing a mycotic aneurysm in case of adjacent infections related to esophageal anastomotic leakages [10, 12]. In most cases, these esophageal anastomotic leakages are iatrogenic or secondary to ischemia or infection.
After multivisceral transplantation, unique additional challenges arise, related to the tissue fragility and heavy immunosuppression, limiting healing response and increasing the risk of infection. In this context, experience from cancer resection has demonstrated that prevention, prompt identification and tailored management are essential to avoid catastrophic outcomes in case of anastomotic leakage [7]. However, traditional management strategies, such as surgical repair or stenting, carry increased risk in immunocompromised patients due to impaired wound healing and increased susceptibility to nosocomial infections [13].
In this context, ENPT may offer several advantages: it provides continuous drainage, promotes granulation tissue formation, and supports localized healing while mitigating surgical morbidity [14]. Yet, ENPT is not without risks and complications, include bleeding, mucosal erosion, stricture formation, and patient discomfort related to repeated endoscopic interventions, have been reported. Consequently, careful patient selection is essential, particularly in the transplant setting. Moreover, close monitoring is mandatory to promptly detect potential adverse events.
While self-expanding metal stents (SEMS) have traditionally been considered the standard endoscopic approach for esophageal leakage, they are associated with risks such as migration, inadequate drainage of infected cavities, and pressure-related mucosal injury. In contrast, ENPT provides active drainage and continuous cavity collapse, resulting in higher closure rates and reduced septic complications. These differences may be particularly relevant in immunosuppressed transplant recipients, where infection control and tissue healing are critical determinants of outcome [15,16]. Of note is that stenosis has been described following both techniques, but can be successfully managed with endoscopic dilatations, as seen in our patient [17].
In particular, the VACStent®, which combines the advantages of a covered stent with vacuum therapy, has shown promising results in case series and allows patients to drink while the stent is in place, increasing the quality of life [18, 19]. While ENPT has been widely documented in colorectal surgery and for postoperative gastric or pancreatic fistulas [18, 19], its use in the setting of multivisceral transplantation has, to our knowledge, not been previously reported.
To the best of our knowledge, this is the first report to describe successful ENPT for an esophageal anastomotic leakage in a patient following multivisceral transplantation, allowing complete resolution of the leakage, even after initial failure of conventional esosponge therapy.
This case contributes to the growing body of evidence supporting ENPT in upper gastrointestinal defects and even support its use in complex immunosuppressed patients. It also highlights the importance of interdisciplinary management involving transplant surgeons, endoscopists, and critical care teams in the care of these patients [20].
However, we have the acknowledge the inherent limitations of single-case studies, including the limited generalizability of these findings, and lack of direct comparison with alternative treatment modalities. Moreover, the favourable outcome observed may reflect patient-specific factors and the expertise of a highly specialized multidisciplinary team. Nevertheless, given that the decision for ENPT was made based on larger experiences from the cancer setting where patients are also more-frail and more-susceptible to infections after induction chemo-(immunotherapy), we believe these findings may be valuable. Nevertheless, larger studies are required to better define indications, timing, and standardized protocols for ENPT in transplant recipients.
Finally, it is also important to consider cost and resource implications. ENPT requires repeated endoscopic procedures, specialized equipment, and experienced endoscopists, which may limit its availability in low-volume or resource-constrained centers. However, the potential reduction in major surgical reinterventions and septic complications, including the loss of the intestinal transplant - requiring lifelong total parenteral nutrition - may offset these costs.
Conclusion
The management of postoperative complications, including esophageal leakage, in multivisceral transplant recipients remains a clinical challenge. Our experience suggests that ENPT may represent a valuable addition in the treatment of esophageal leakage in these immunocompromised high-risk patients in whom surgical reintervention carries substantial morbidity.
Conflicts of Interest
None.
Acknowledgement
We thank the patient and her family, without whom the discussion of this case would not have been possible. We also thank the faculty members and allied health personnel of the Departments of Anesthesiology, Intensive Care and Thoracic Surgery of the University Hospitals of Leuven, who provided and cared for this patient.
Funding
None.
Article Info
Article Type
Case ReportPublication history
Received: Tue 20, Jan 2026Accepted: Mon 23, Feb 2026
Published: Mon 01, Jun 2026
Copyright
© 2023 Philippe Nafteux. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.TCR.2026.01.01
Figures & Tables
References
1. Di Cocco
P, Martinino A, Lian A, Johnson J, Spaggiari M et al. (2024) Indications for
multivisceral transplantation: A systematic review. Gastroenterol. Clin. North
Am, 53: 245-264. [Crossref]
2. Russell
ND, Dattilo JB (2022) Intestinal and multivisceral transplantation. Surgery
(Oxford). [Crossref]
3. Dasyam
AK, Borhani AA, Tirukkovalur NV, Cruz Jr. RJ (2023) Intestinal and
multivisceral transplantation: Complications. Radiol Clin. North Am, 61:
871-887. [Crossref]
4. Canovai
E, Ceulemans LJ, Gilbo N, Duchateau NM, Hertogh GD et al. (2021) Multivisceral
transplantation for diffuse portomesenteric thrombosis: Lessons learned for
surgical optimization. Front Surg, 8: 645302. [Crossref]
5. Ceulemans
LJ, Braza F, Monbaliu D, Jochmans I, De Hertogh G et al. “The Leuven
immunomodulatory protocol promotes T-regulatory cells and substantially
prolongs survival after first intestinal transplantation.” Am J Transplant,
16: 2973-2985. [Crossref]
6. Gilshtein
H, Bahouth H, Kluger Y (2021) Esophageal perforation: A review of the
literature and a proposed management algorithm. Am J Surg, 222: 618-627.
7. Vanstraelen
S, Coosemans W, Depypere L, Mandeville Y, Moons J et al. (2023) Real-life
introduction of powered circular stapler for esophagogastric anastomosis:
Cohort and propensity matched score study. Dis Esophagus, 36: doac073. [Crossref]
8. Weidenhagen
R, Hartl WH, Gruetzner KU, Eichhorn ME, Spelsberg F et al. (2010) Anastomotic
leakage after esophageal resection: New treatment options by endoluminal vacuum
therapy. Ann Thorac Surg, 85: 1700-1706. [Crossref]
9. Struyve
M, De Vloo C, Van Veer H, Depypere L, Nafteux P et al. (2019) Endoscopic
vacuum-assisted closure therapy for the treatment of oesophageal anastomotic
leaks,” Acta Gastroenterol Belg, 82: 529-531. [Crossref]
10. Ceulemans
LJ, Jochmans I, Monbaliu D, Verhaegen M, Laleman W et al. (2015) “Preoperative
arterial embolization facilitates multivisceral transplantation for
portomesenteric thrombosis. Am J Transplant, 15: 2963-2969. [Crossref]
11. Muylle
E, Van De Winkel N, Hennion I, Dubois A, Thorrez L et al. (2024) Abdominal wall
closure in intestinal and multivisceral transplantation: A state-of-the-art
review of vascularized abdominal wall and nonvascularized rectus fascia
transplantation. Gastroenterol Clin North Am, 53: 265-279. [Crossref]
12. Costa G,
Parekh N, Osman M, Armanyous S, Fujiki M et al. (2019) Composite and
multivisceral transplantation: Nomenclature, surgical techniques, current
practice, and long-term outcome. Surg Clin North Am, 99: 129-151. [Crossref]
13. Loske G,
Müller CT, Scholz T, Büsing M, Reimer S (2017) Endoscopic vacuum therapy for
esophageal perforation. Surg Endosc, 31: 4352-4359.
14. Loske G
Endoscopic vacuum therapy for gastrointestinal leaks and perforations. Gastrointest
Endosc Clin N Am, 30: 567-586.
15. Mandarino
FV, Barchi A, D'Amico F, Fanti L, Azzolini F et al. Endoscopic vacuum therapy
(EVT) versus self-expandable metal stent (SEMS) for anastomotic leaks after
upper gastrointestinal surgery: Systematic review and meta-analysis. Life
(Basel), 13: 287. [Crossref]
16. do Monte
Junior ES, de Moura DTH, Ribeiro IB, Hathorn KE, Farias GFA et al. (2021)
“Endoscopic vacuum therapy versus endoscopic stenting for upper
gastrointestinal transmural defects: Systematic review and meta-analysis. Dig
Endosc, 33: 892-902. [Crossref]
17. Adamenko
O, Ferrari C, Seewald S, Schmidt J Prophylactic endoluminal vacuum therapy
after major gastrointestinal surgery: A systematic review. Updates Surg,
74: 1177-1186. [Crossref]
18. Kühn F,
Hasenhütl SM, Hofmann FO, Wirth U, Drefs M et al. Endoscopic vacuum therapy for
left-sided colorectal anastomotic leak without fecal diversion. Dis Colon
Rectum, 65: 421-428. [Crossref]
19. Bemelman
WA, Arezzo A, Banasiewicz T, Brady R, Espín-Basany E et al. Use of
sponge-assisted endoluminal vacuum therapy for the treatment of colorectal
anastomotic leaks: Expert panel consensus. BJS Open, 6: zrac123. [Crossref]
20. Samela
K, Fennelly E, Brosnan M, Robinson J Interdisciplinary approach to the
management of intestinal transplant recipients: Evaluation, discharge, and
lifetime management. Prog Transplant, 15: 54-59. [Crossref]