Efficiency of Connected Health Telemonitoring Platform for Patients with High Blood Pressure
A B S T R A C T
Background: Chronic diseases are expected to double their current incidence in people over 65, before by 2030. Cardiovascular diseases, such as ischemic heart disease and heart failure, are the most common cause of morbidity and mortality in developed countries and high blood pressure is the most prevalent risk factor. Telemedicine collects data, shares information and provides clinical care, education, public health and remote administrative services. Telehealth and specially connected health platforms, have the potential to improve the health care system, reduce costs and increase patient satisfaction.
Methods: During 2018, 111 patients with high blood pressure (81 (73%) men and 30 (27%) women with an average age 58,4 years) were selected and followed for 12 months. All patients included in the telemonitoring program, received the Connected Health application on their smartphone and a bluetooth device to measure blood pressure. The application reinforces education about the disease, treatment compliance, blood pressure monitoring and in case of decompensation, generates alarms that trigger a response by the medical team with video consultation.
Results: To analyse the difference in blood pressure (systolic and diastolic), we calculate the average of the first (when patients added to the program) and last 30 measurements after the 12-month follow-up. We observed a reduction of 5,7 mmHg (4%) in systolic and 4 mmHg (5%) in diastolic blood pressure (p <0.05). The use of the connected health platform avoided 3,2% of costs (Blood Pressure Holter and outpatient visits) in one year. The patient satisfaction analysed with the Net Promoting Score of the services implicated increased 2.2 points during the study period.
Conclusion: A telemonitoring platform for patients with high blood pressure, based on health education, treatment compliance, blood pressure monitoring and early detection of decompensation, improves blood pressure figures, reduce costs and increase patient satisfaction.
Keywords
Telemedicine, connected health, telemonitoring, hypertension
Introduction
It is estimated that in 2050, about 35% of our population will exceed 65 years and chronic diseases are expected to double their current incidence in people over 65, before by 2030. Cardiovascular diseases, such as ischemic heart disease and heart failure, are the most common cause of morbidity and mortality in developed countries and high blood pressure is the most prevalent risk factor. More than half of these admissions are theoretically avoidable because the main cause of cardiac decompensation is poor therapeutic compliance (abandonment of drugs and hygienic and dietary measures, due to lack of knowledge or motivation and lack of support from family members and caregivers) and poor control of blood pressure [1].
Telemedicine collects data, shares information and provides clinical care, education, public health and remote administrative services. Connected health platforms have the conjunction of digital health (eHealth) and mobile health (mHealth), conforms the so-called telehealth, which has the potential to help transform the health care system, reduce costs and increase patient quality and satisfaction [2]. Mobile devices and applications create the digital environment to facilitate access, delivering medical care anywhere and improving user experience. Patients can use sensors that measure a large number of variables (from blood pressure, heart rate, temperature, weight, to daily exercise and their perceived state of health), allowing doctors to remotely monitor their health, providing reminders to help them keep track their care. This digital channel can also be used to collect large amounts of high-quality, real-time data on medication adherence, symptoms and care plan compliance. This technology also can build a different relationship with the patient, focused on their needs, more transparent and continuous with twenty-four hours a day follow-up, where the user enjoys much more information, participation and autonomy [3].
There is sufficient evidence that telemedicine improves the health of the population, reduces healthcare costs and improves the client's experience in health care [4]. That is why different scientific societies already recommend the use of telemedicine for better health control, such as the American Heart Association [2]. Previous telemonitoring studies carried out in our hospitals and the previous considerations led us to the creation of a telemonitoring platform called Connected Health [5]. This platform is based on an interactive telemedicine system that combines ambulatory telemonitoring of different health variables (blood pressure and heart rate). This platform has also an application for smartphone, with educational instruments to improve the knowledge of the disease and motivational support (for controlling variables related to health and adherence program of taking medication), added to a telecare support by medical and nursing staff, who can contact by video consultation through the same application. The main objective of this study is to analyse if the Connected Health improves the blood pressure control, and at the same time, the use of health resources, economic costs and the quality of life and satisfaction of these chronic patients.
Materials and Methods
I Population
The program applies to the entire network of 4 hospitals and other healthcare centers of Sanitas in Spain. During 2018, 111 patients with high blood pressure under pharmacological treatment were selected and followed for 12 months.
The study was approved by the Ethics and Clinical Research Commission of the center and all patients gave informed written consent to participate. All patients met both of the following criteria were available to use wearables (BPM-200) and the mobile app (Salud Conectada iOS/Android app), and if needed, an educational training was received.
II Connected Health
Connected health platform is a CE class I medical device mobile application, for telemonitoring with bluetooth connected wearables adjusted to the user case and video consultation. All patients included in the program receive the Connected Health application on their smartphone and devices to measure continuous and real-time health variables (blood pressure and heart rate). Sanitas also provides the software, technology, training, services and care related to the program, free of charge and there is no cost added to the patient neither the doctor as users of the project.
The Patient always knows through the application in real time all the information that is collected. All information is stored in the electronic medical record, where the healthcare staff can access the measured parameters. There is also the option, if the patient so desires and gives explicit consent, to allow third parties of his or her trust (such as caregivers or family members) to access their information and carry out real-time monitoring. A 24/7 assistance support allows the patient to be warned in the event that the system produces an alert in view of its parameters. The application allows to create warning alarms of measures of health variables, taking medication and to confirm it.
In case of detection of an altered value, the application automatically will notify the healthcare team who will contact the patient via video consultation, allowing the early detection and evaluation of decompensations, through the two-way communication established between the patient and the doctor. The application includes educational material, which is based on knowledge of the disease, rules of self-care, vaccination, reinforce therapeutic compliance and early detection of decompensations.
III Measurements
In order to understand clinical effectiveness of this platform we used patient demographics variables and blood pressure (systolic and diastolic) measured initially when patients added to the program and after the 12-month follow-up. To analyse the economic impact, we calculate the cost of the average tests (two Blood Pressure Holter) and consultations (two outpatient visits) the patients usually need during 12 months, and he patient satisfaction was analysed with the Net Promoting Score (NPS) of the services implicated in the study. To protect all information related to the Patient, different security measures were adopted, technical and organizational, including encryption and authentication tools, and personal data was stored in secure networks.
IV Statistical Analysis
Comparison between Blood pressure (systolic and diastolic) measures, initially and after the 12-month follow-up, was done with Student's t test for independent data. All analyses were performed using the statistical significance level considered for calculation of the sample size (α=.05) with SPSS for Windows (version 12.0).
Results
We analysed 111 patients, 81 (73%) were men and 30 (27%) women. The average age of the sample was 58,4 years. One of the hospitals (CIMA) enrolled 47% of the participants, but no differences were observed between them. To analyse the difference in blood pressure (systolic and diastolic), we calculate the average of the first (when patients added to the program) and last 30 measurements after the 12-month follow-up. We observed a reduction of 5,7 mmHg (4%) in systolic and 4 mmHg (5%) in diastolic blood pressure (p<0.05) (Figure 1).
To analyse the economic impact for the organization and the patient, we calculate the average tests (two Blood Pressure Holter) and consultations (two outpatient visits) the patients usually need during the 12 months study process. The use of the connected health platform avoided 3,2% of costs in one year. To analyse the patient satisfaction, we calculate the Net Promoting Score (NPS) of the services implicated in the study during the program (Figure 2), which increased 2.2 points during the study period.
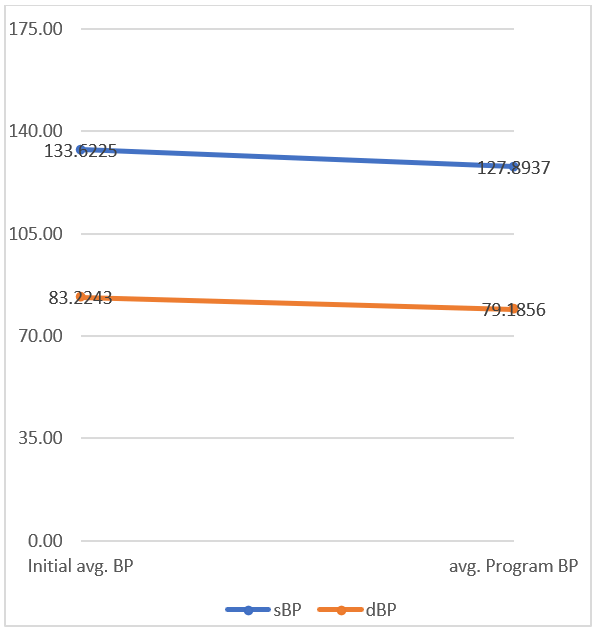
Figure 1: Blood pressure (systolic sBP and diastolic dBP) difference after 12-month follow-up.
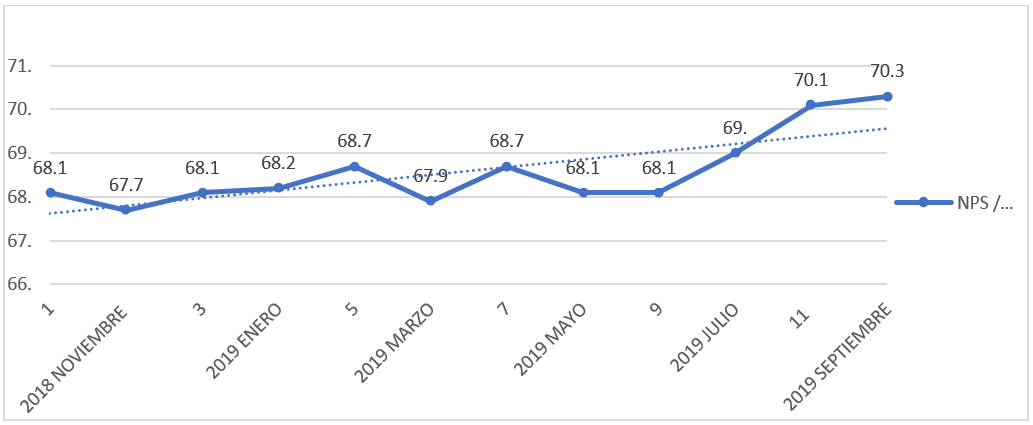
Figure 2: Net Promoting Score (NPS) evolution during 12-month follow-up.
Discussion
This study evaluates how digital technologies like a telemonitoring platform for patients with high blood pressure, based on health education, treatment compliance, blood pressure monitoring and early detection of decompensation, improves blood pressure figures, reduce costs and increase patient satisfaction. The effectiveness of outpatient follow-up programs for patients with cardiovascular diseases is already known. They are based on health education and they can reinforce disease knowledge and boost self-care like therapeutic adherence and help to detect early decompensations [1]. Home telemonitoring has the double advantage of providing monitoring and encouraging patient participation in the management of their own disease [6]. Several studies have shown that telemonitoring improves the control of chronic diseases such as blood pressure, overweight, diabetes and heart failure [7-12].
The interest in telemedicine is increasing, thanks to technological advances and the greater availability of easy-to-use equipment, which increase the acceptance and satisfaction of patients to acquire and use these technologies. Net Promoter Score (NPS) measures customer experience and predicts business growth. This proven metric transformed the business world and now provides the core measurement for customer experience management programs the world round. In healthcare organizations isn’t extended as in another business corporations. But there are hospitals and clinics that they are using it as a powerful tool to measure patient satisfaction. This program helped to increase patient satisfaction, probably because allows to descend follow-up consultations and tests, and increases the availability of clinical staff, potentially reducing waiting lists. The medical staff and patient engagement with the Telehealth platform was high, thanks to an educational process with monthly workshops with all the stakeholders involved.
Theoretically this program could absorb 25% of medical consultation and tests manageable in output medical practice, can improve costs savings to 5% and reduce waiting lists. Based on telehealth efficiency, in many countries like US, there are already reimbursement models for telemonitoring platforms [13]. This study has certain limitations and should be interpreted with caution. It has included only patients with grade I hypertension (less than 140 mmHg) who received a first stage treatment, therefore, these results cannot be extrapolated to patients in other stages of the disease, although due to the increased use of drugs, they could even have more significant changes. This study has no control group and has not analysed individual treatments, but the 4-5% blood pressure reduction is comparable to first step of drug introduction (Angiotensin-converting-enzyme inhibitors ACEi plus Diuretics) in low grade hypertension patients [14].
Conclusion
This study analyses the efficiency of a telemonitoring platform for patients with high blood pressure, based on health education, treatment compliance, blood pressure monitoring and early detection of decompensation, and shows an improvement of blood pressure figures, reduction of costs and an increase of patient satisfaction.
Conflicts of Interest
None.
Funding
None.
Article Info
Article Type
Research ArticlePublication history
Received: Thu 21, May 2020Accepted: Sat 06, Jun 2020
Published: Fri 12, Jun 2020
Copyright
© 2023 Cèsar Morcillo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JICOA.2020.03.09
Figures & Tables
References
- Aguado O, Morcillo C, Delàs J, Rennie M, Bechich S et al. (2010) Long-term Implications of a Single Home-Based Educational Intervention in Patients With Heart Failure. Heart Lung 39: S14-S22. [Crossref]
- Schwamm LH, Chumbler N, Brown E, Fonarow GC, Berube D et al. (2017) Recommendations for the Implementation of Telehealth in Cardiovascular and Stroke Care: A Policy Statement From the American Heart Association. Circulation 135: e24-e44. [Crossref]
- Morcillo C, González JL (2020) Nuevas tecnologías digitales en la práctica médica. Med Clin Barc 154: 20-22.
- Tuckson RV, Edmunds M, Hodgkins ML (2017) Telehealth. N Engl J Med 377: 1585-1592. [Crossref]
- Mirón Rubio M, Ceballos Fernández R, Parras Pastor I, Palomo Iloro A, Fernández Félix BM et al. (2018) Telemonitoring and Home Hospitalization in Patients With Chronic Obstructive Pulmonary Disease: Study TELEPOC. Expert Rev Respir Med 12: 335-343. [Crossref]
- Stergiou GS, Nasothimiou EG (2011) Hypertension: Does Home Telemonitoring Improve Hypertension Management? Nat Rev Nephrol 7: 493-495. [Crossref]
- McManus RJ, Mant J, Franssen M, Nickless A, Schwartz C et al. (2018) Efficacy of Self-Monitored Blood Pressure, With or Without Telemonitoring, for Titration of Antihypertensive Medication (TASMINH4): An Unmasked Randomised Controlled Trial. Lancet 391: 949-959. [Crossref]
- Ciemins EL, Arora A, Coombs NC, Holloway B, Mullette EJ et al. (2018) Improving Blood Pressure Control Using Smart Technology. Telemed J E Health 24: 222-228. [Crossref]
- Lee CH, Cheung B, Yi G, Oh B, Oh YH (2018) Mobile Health, Physical Activity, and Obesity: Subanalysis of a Randomized Controlled Trial. Medicine (Baltimore) 97: e12309. [Crossref]
- Everett E, Kane B, Yoo A, Dobs A, Mathioudakis N (2018) A Novel Approach for Fully Automated, Personalized Health Coaching for Adults with Prediabetes: Pilot Clinical Trial. J Med Internet Res 20: e72. [Crossref]
- Koehler F, Koehler K, Deckwart O, Prescher S, Wegscheider K et al. (2018) Efficacy of Telemedical Interventional Management in Patients With Heart Failure (TIM-HF2): A Randomised, Controlled, Parallel-Group, Unmasked Trial. Lancet 392: 1047-1057. [Crossref]
- Stehlik J, Schmalfuss C, Bozkurt B, Nativi Nicolau J, Wohlfahrt P et al. (2020) Continuous Wearable Monitoring Analytics Predict Heart Failure Hospitalization: The LINK-HF Multicenter Study. Circ Heart Fail 13: e006513. [Crossref]
- Berridge C (2018) Medicaid Becomes the First Third-Party Payer to Cover Passive Remote Monitoring for Home Care: Policy Analysis. J Med Internet Res 20: e66. [Crossref]
- Miró O, Rosselló X, Gil V, Martín Sánchez FJ, Llorens P et al. (2019) 2018 ESC/ESH Guidelines for the management of arterial hypertension. Rev Esp Cardiol 72: 160.