Conventional Technique with Modernisation: Non-Descent Vaginal Hysterectomy with Removal of Largest Ovarian Tumor Through Same Route in Tribal Belt of India
A B S T R A C T
Various surgical approaches such as vaginal, abdominal, laparoscopic and robotic assisted laparoscopic hysterectomy are considered for hysterectomy and risk factors and associated morbidity determines the selection of the surgical procedure. The available healthcare infrastructure also determines that surgical approach considered for the patients and needs some customisation. In this case report, the case of Non-Descent Vaginal Hysterectomy along with the right sided & left sided salpingo-oophorectomy in rural tribal belt tertiary healthcare center in Dahod, Gujrat, India is reported. Total weight of the tumor removed measured 6.5Kg out of that 6.1Kg was fluid and 400 Gram solid component. On histopathology report confirmed serous cystadenoma. There was no stitch, no scar performed, and this total vaginal surgery was successful.
Keywords
Hysterectomy, non-descent vaginal hysterectomy, uterine tumor, salpingo-oophorectomy
Introduction
A substantial number of women undergo hysterectomy annually, and 70 % of hysterectomies are performed for benign indications, including leiomyoma, adenomyosis, severe dysmenorrhea and uterine prolapse. Various surgical approaches such as vaginal, abdominal, laparoscopic and robotic assisted laparoscopic hysterectomy are considered for hysterectomy and risk factors and associated morbidity determines the selection of the surgical procedure. The available healthcare infrastructure also determines that surgical approach considered for the patients and needs some customisation [1, 2].
In this case report, the case of Non-Descent Vaginal Hysterectomy along with the right sided & left sided salpingo-oophorectomy in rural tribal belt tertiary healthcare center in Dahod, Gujrat, India.
Case Report
In a rural tribal belt of Dahod, Gujrat, 42-year-old married women visited for abnormally big belly. The patient was on a very heavy side of the body weight weighing 100.3 kg, height 150 cm and BMI 44. The patient had complained of increasing abdominal swelling since past 3 to 7 months. The patient had maintained regular menstrual cycles and had no other complaints. The laboratory reports including tumor markers (CA 125, AFP, B HCG) were normal and upon clinical examination, there was a suspicion of pelvic mass. On per abdomen 28 to 32 weeks size cystic mass arising from pelvis was observed. The radiographic examination by CECT scan revealed presence of ovarian tumor (Figure 1).
Large well defined thin walled peripherally enhancing fluid density cystic lesion with smooth margins was seen occupying almost the entire abdomino-pelvic region. It measured approximately 26.0 × 29.7 × 30.5 cm (APXTRX CC) in size. It was extending superiorly up to inferior border of L2 vertebrae and laterally up to both flanks. It was compressing and displacing the bowel loops laterally and posteriorly. No solid component or internal septa was seen. Neither calcification nor hemorrhage was observed. Right ovary was seen separately from the lesion. Lesion was in close approximation with left ovary. The decision to surgically remove the tumor was taken and patient was operated on 09th July 2021 using Ligasure Vessel Sealer (manufactured by Medtronic India Pvt Ltd.).
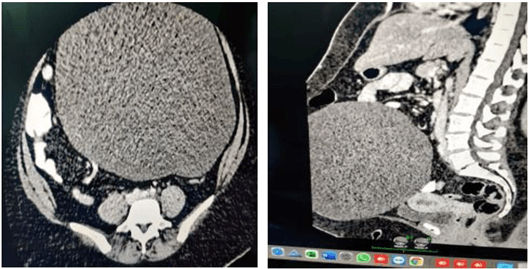
Figure 1: CT Scan report.
The surgical approach undertaken was Non-Descent Vaginal Hysterectomy (VH) along with the right sided & left sided salpingo-oophorectomy.

Figure 2: Surgical steps.
The surgery was conducted under general anaesthesia using video Laryngoscope. Hydraulic leg stirrup was mounted so as to permit the simultaneous abduction, lithotomy and easy adjustment of position possible during surgery. Patient was highly obese and in order to reduce any post-surgical complications decision as Non-Descent Vaginal Hysterectomy (NDVH) with bilateral salpingo-oophorectomy was undertaken. Bupivacaine a local anaesthetic solution for injection was used to anaesthetize or numb the surgical area. Hydro-dissection with peri-cervical block with bupivacaine, followed by a and p-pouch opening, dissect uterosacral + cardinal + uterine art with Ligasure® vessel sealer was followed. Amputation of cervix, followed by upper pedicle with bilateral-salpingo - oophorectomy was undertaken using Ligasure® device 23cm Maryland. Right sided oophorectomy was achieved with controlled suction and simultaneously seal and cut pedicle with Ligasure® was undertaken (Figure 2).
Total weight of the tumor removed measured 6.5Kg out of that 6.1Kg was fluid and 400Gram solid component. On histopathology report confirm serous cystadenoma. There was no stitch, no scar performed, and this total vaginal surgery was successful. The surgical time was 2 hours, recovery was uneventful. Patients was hospitalised for 2 days and was discharged.
Discussion
Benign ovarian masses include functional cysts and tumors. Treatment varies depending on the patient's reproductive status. Most functional cysts and benign tumors are asymptomatic. Masses are usually detected incidentally, and it was true in this patient too who visited the hospital for expanding belly with no other symptoms. The patient was extremely obese, could not adjust for MRI and therefore based on the CTCE the surgical decision was finalised. In this patient, we had to consider all possible post-surgical complications that can occur due to obesity. Open abdominal surgery could have led for post-operational hernia and longer hospital stay and therefore, based on the ACOG guidelines, Cochrane review, vaginal hysterectomy (NDVH) was considered. Vaginal hysterectomy is associated with a shorter duration of hospital stay, speedier recuperation, fewer unspecified infections or febrile episodes than abdominal hysterectomy as well as reported with fewer complication with scarless procedures [3].
We used video laryngoscope for intubation and hydraulic legs stirrups for simultaneous abduction and lithotomy position. We considered using Ligasure device from Medtronic. It is an advanced surgical tool used for sealing blood vessels. It can be used to seal blood vessels up to 7 mm in diameter and is frequently utilized with many laparoscopic procedures. The effective use of this advanced sealing method has significantly decreased the anaesthesia duration, reduced bleeding, inflammation and pain. Therefore, in order to minimise any post-surgical complications, we decided to use Ligasure® for this surgery [4]. The results have been stunning. We initially carried the total hysterectomy and then the tumor along with the left-side oophorectomy and could remove the tumor weighing 6.5 kg with ease. There were no scars, no excessive bleeding and was relatively pain free. Patient had an uneventful recovery. This least minimally invasive procedure is of immense importance to reduce morbidity, extended hospitalisation and economics for the patients. The removal such a big size tumor was reported in the local and national papers including India book of record, and Asia book of record and this was achieved in the tribal belt of India.
Our literature search for similar case from various search engines such as PUBMED, google etc. revealed that so far there have been no reports of removal of such large ovarian tumors by vaginal hysterectomy. Majority specialists have approached big tumor resection via abdominal route for large tumors. This report is the testimony of successful removal of abnormally high sized ovarian tumors with minimal blood loss, no scaring and no stitches. The procedure has been safe with minimal pain early recovery in patients. Total hysterectomy procedure can be considered in similar cases. It is also economical for the patients and reduces healthcare costs.
Acknowledgement
Authors would like to acknowledge the writing assistance provided by Dr. Manjusha Rajarshi, Mumbai in preparing this case report.
Article Info
Article Type
Case ReportPublication history
Received: Fri 23, Dec 2022Accepted: Fri 06, Jan 2023
Published: Sat 04, Feb 2023
Copyright
© 2023 Rahul Kumar M Padval. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.CROGR.2022.02.02
Figures & Tables
References
1. (2009) ACOG
Committee Opinion No. 444: choosing the route of hysterectomy for benign
disease. Obstet Gynecol 114: 1156-1158. [Crossref]
2. Lee SH, Oh SR, Cho
YJ, Han M, Park JW et al. (2019) Comparison of vaginal hysterectomy and
laparoscopic hysterectomy: a systematic review and meta-analysis. BMC Womens
Health 19: 83. [Crossref]
3. Sarada Murali M, Khan A (2019) A Comparative Study of Non-descent Vaginal Hysterectomy and Laparoscopic Hysterectomy. J Obstet Gynaecol India 69: 369-373. [Crossref]
4. Carlin GL, Bodner Adler B, Husslein H, Ritter M, Umek W et al. (2021) The effectiveness of surgical procedures to prevent post-hysterectomy pelvic organ prolapse: a systematic review of the literature. Int Urogynecol J 32: 775-783. [Crossref]