Complex Ankle Fractures, Presentation of 3 Cases and Review of the Literature
Complex Ankle Fractures, Presentation of 3 Cases and Review of the Literature
A B S T R A C T
Ankle fractures represent a significant percentage of all fractures, and there is currently an increased incidence, both among the elderly population with associated comorbidities and among young patients with high-energy traumas. These fractures have an inherent risk of complications. In this connection, it is crucial that we turn our attention to soft tissue injuries, with wound infection as the main complication in this category. The last objective of this study is to highlight the possible derived complications in complex ankle fractures, and to explain the advantages of the use of different fixation devices, through the presentation of three clinical cases treated in our center. We conclude in order to prevent or reduce the complications resulting from the direct surgical treatment of high-energy trauma in the distal end of the tibia, it is essential to properly manage the soft tissue based on the type of lesion and the characteristics of the patient.
Keywords
Ankle, open fractures, soft tissues, external fixation
Introduction
Ankle fractures represent approximately 10% of all fractures, and there is currently an increased incidence, both among the elderly population with associated comorbidities and among young patients with high-energy traumas, which leads to complex fractures [1]. There are different therapeutic options that can be taken into consideration in this type of fractures: 1) immediate definitive fixation; 2) delayed surgical stabilization after non surgical immobilization and 3) definitive fixation after temporary surgical stabilization. The decision will be determined by the “personality of the fracture”, and in order to define it, it is necessary to understand the mechanisms that produced it and to identify potential risk factors [2-4].
These fractures have an inherent risk of complications, such as malunion or pseudoarthrosis, implant failure, and soft tissue injuries, with wound infection as the main complication in this last category [1, 2].
Based on these considerations, we discuss the following topics:
i. Best time for surgical intervention: Is delayed surgery associated with a higher involvement of soft tissue? Does infection associated with prolonged immobilization create a predisposition for poorer results [5]?
ii. Fixation method: Is it sensible to use open reduction and internal fixation universally? What fixation method gets better results and what are the factors that lead to a good outcome [6]?
iii. What is the degree of repercussion of soft tissue involvement on the final result of these lesions? What are the best protocols for the management of soft tissue?
The last objective of this study is to highlight the possible derived complications of soft tissue in complex ankle fractures, and to explain the advantages of the use of different fixation devices, through the presentation of three clinical cases treated in our center.
Case Report
We present three clinical cases of patients between 46 and 60 years old with complex ankle fractures and the management for each of them.
Case 1
The patient is a 46-year-old man who had suffered a workplace accident in which he fell from 3 meters on his right lower limb, and he presented a Gustilo grade 2 bimalleolar open fracture and dislocation of the ipsilateral ankle. The radiological tests revealed a medial malleolus and anterior tibial fracture associated with a comminuted fracture in the distal third of the fibula (Figure 1).

Figure 1: Medial malleolus and anterior tibial fracture associated with a comminuted fracture in the distal third of the fibula.
Open reduction was carried out with antibiotic coverage (treatment according to hospital protocol: intravenous cefazolin and gentamicin) and emergency spinal anaesthesia in the operating room. A direct approach was adopted through the longitudinal extension of the open fracture wound on the posterior end of the fibula, which revealed a comminuted fracture of the distal epiphysis associated with complete rupture of the distal part of the Achilles tendon. An internal fixation of the fibula was performed with a neutralization plate with 5 screws and 2 interfragmentary screws; and the tibia was fixated with 2 partially threaded cancellous screws and compression on the internal malleolus and another anteroposterior screw for the anterior fragment, after a closed reduction of both fragments with direct fluoroscopic control (Figure 2).
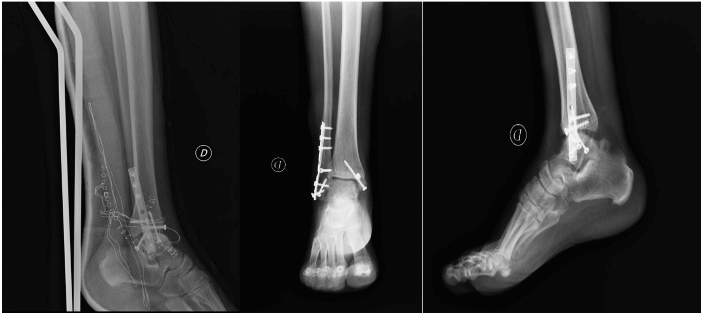
Figure 2: Postoperative RX images.
Finally, an end to end Kessler suture of the Achilles tendon was performed. Given the low contamination of the wound, a direct layered closure of the incision was decided, which showed correct tension of the soft tissue; and a long leg splint was placed in resting equinus with periodic controlled dorsal flexion to manage the associated lesion of the tendon.
The patient remained in hospital with intravenous antibiotic treatment and periodic wound cleansing, without blistering lesions and with a correct evolution of the wounds, and he was discharged 5 days after the operation and was monitored by his mutual insurance company. 20 days later, he was referred to our center by his mutual insurance company for the assessment of a possible superinfection of the surgical wound because the patient presented a slight dehiscence on the area of the Achilles tendon suture, with surrounding granulation tissue. The clinical examination and the analyses ruled out the presence of infection at that time, and a dry treatment of the wound was indicated with prophylactic oral broad-spectrum antibiotics. A good evolution of the wound was observed.
Case 2
The patient is a 60-year-old man, without relevant history, who had a traffic accident with multiple trauma and comminuted diaphyseal fracture of the left femur, comminuted pilon fracture of the left tibia associated with fracture of the fibula in the medial and proximal thirds, and fracture-subluxation of the ipsilateral calcaneus with involvement of the anterior tuberosity, particularly in its super-external area (Figure 3). An emergency treatment was implemented with antibiotic coverage and spinal anaesthesia, and Hoffmann external fixators were applied on the femur and the tibia with three proximal pins on the tibial diaphysis and a transfixion transcalcaneal pin, followed by an external fixation of the femur, which achieved a correct intraoperative reduction of the fractures.
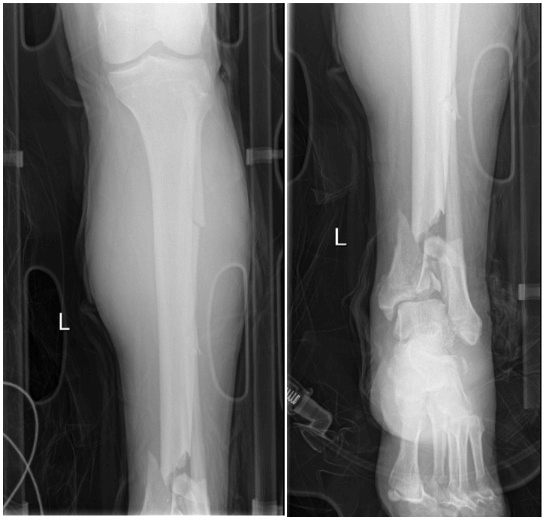
Figure 3: Complex distal tibia fracture.
A CT scan was requested after an emergency reduction in order to study the ankle fracture and prepare an adequate management for its treatment (Figure 4). Definitive surgery was performed 9 days after improvement of the soft tissue was observed. During that period, the patient presented inflammation and edemas on the limb, with the appearance of serous blisters that were treated with dry healing and physical measures, such as elevation of the limb with a Braun splint and cryotherapy.
In the definitive surgery of the fracture, a closed reduction was performed on a traction table with radioscopic control of the femur fracture through osteosynthesis with a long intramedullary cervical-diaphyseal nail and 3 titanium cerclage wires; together with open reduction via anterior ankle and placement of a 3.5mm LCP anterolateral distal tibial plate with distal blocking screws that provide support for the joint surface, and three partially threaded compression screws for the Volkmann fragment and the medial malleolus. During the closure, no tension was observed in the soft tissue, and primary closure of the surgical incision was performed with drainage on the femoral fracture, but not on the ankle fracture (Figure 5).
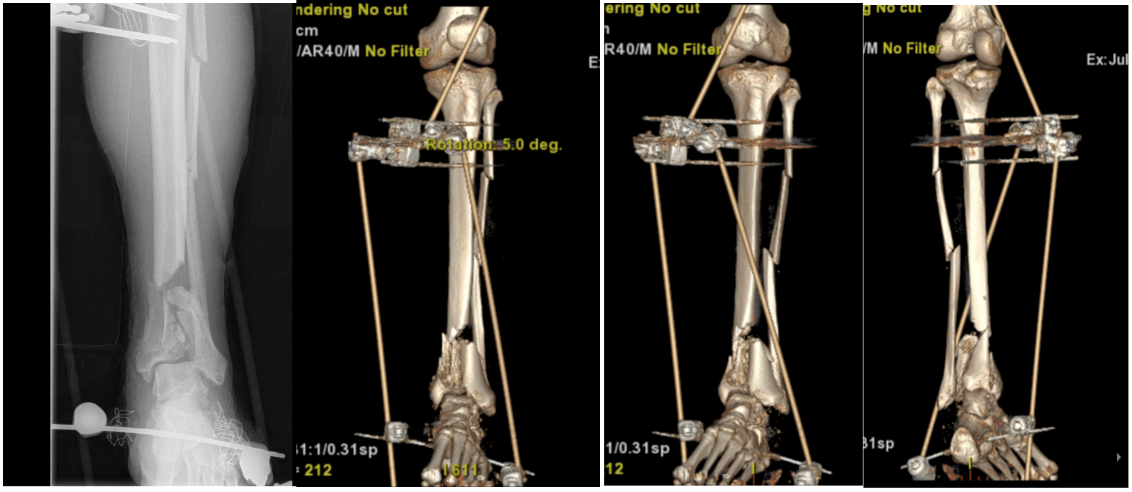
Figure 4: CT Scan after external fixation procedure.
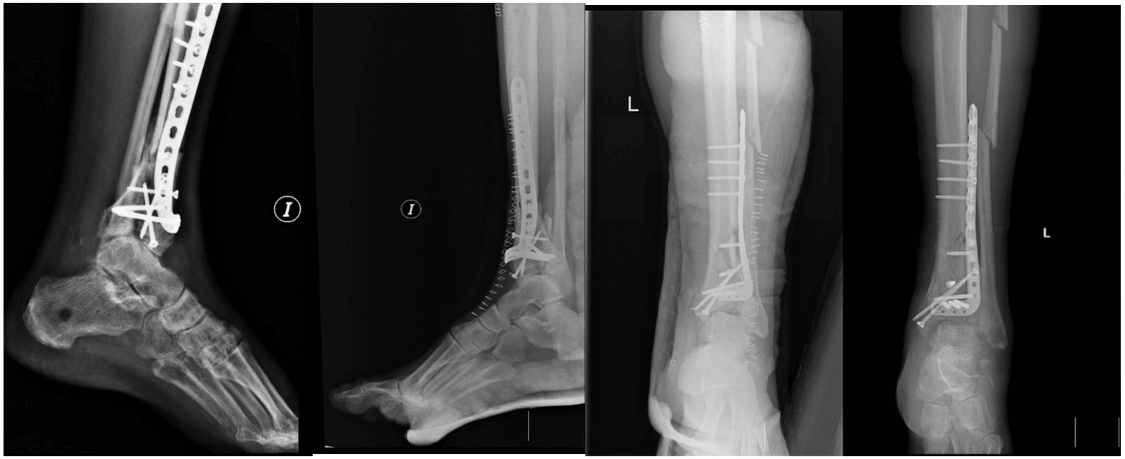
Figure 5: Postoperative Rx images.
The patient was hospitalized for 15 days, with antibiotic treatment and regular healing, and he presented a 2x2cm eschar on the medial region that was treated at first with dry healing with topical povidone-iodine and povidone-iodine dressings, and enzymatic debridement was started with collagenase ointment 4 days after the surgery, followed by two procedures for physical debridement with a scalpel, which revealed granulation tissue on the bottom of the wound and bleeding edges. Two months later, the patient presented a good evolution of the wounds, with granulation tissue and without dehiscence, and he still did not show epithelialization, which appeared three months after the surgery, when he could stand on that leg without load bearing.
Case 3
The patient is a 51-year-old woman who fell from a horse and had a bilateral ankle fracture. She presented a Gustilo grade 3 open fracture-dislocation that affected the anterior and posterior left tibial malleolus, associated with closed fracture of the distal third and comminuted fracture of the right fibula (Figure 6).
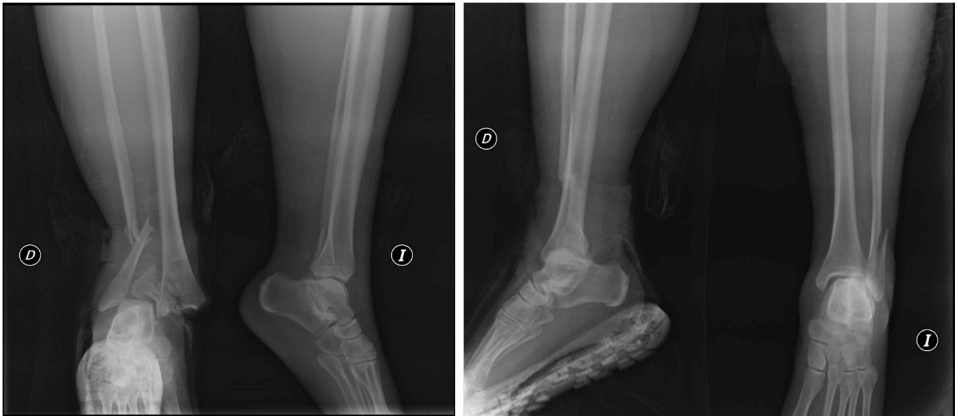
Figure 6: Bilateral ankle fracture.
After administrating the antibiotic treatment that was part of the hospital protocol, an emergency procedure was carried out in a first stage with spinal anaesthesia and placement of a Hoffmann external fixator on the left ankle with two proximal pins on the diaphyseal region of the tibia and two distal pins (a transfixion pin through the calcaneus and another one on the first metatarsal bone), which achieved a congruent reduction in the ankle with intraoperative fluoroscopic control. Given the presence of a contaminated wound associated with the open fracture, and the significant inflammation of the limb with the appearance of blistering lesions with haemorrhagic characteristics, a primary suture was not performed, and the wound was treated with an antibiotic ointment that used nitrofurazone as an active ingredient. At the same time, a closed reduction and internal fixation of the right ankle were performed with a one-third tubular plate and a transsyndesmotic screw (Figure 7).
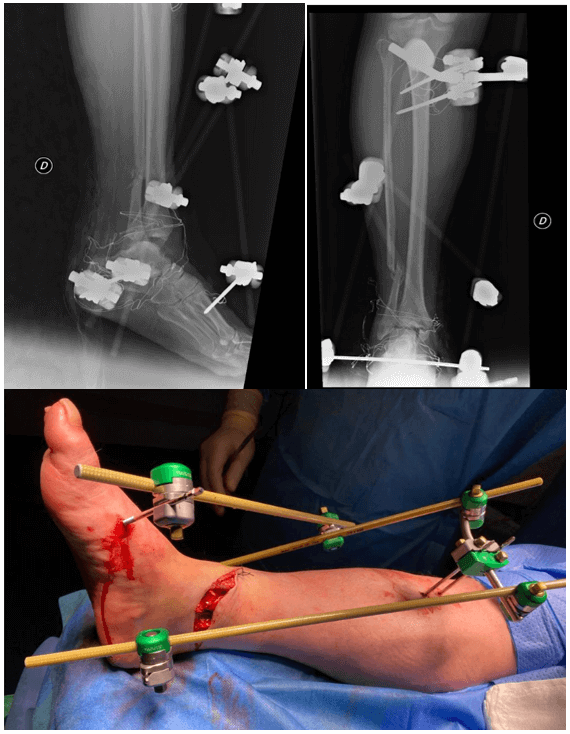
Figure 7: External fixation procedure.
A definitive surgical operation was planned in a second stage, after observing an improvement of the soft tissue, and it was performed 15 days after the lesion, without the presence of blisters or edema, but with a necrotic eschar on the site of the open fracture. In this second stage, an internal fixation of the left ankle was applied with a plate on the fibula after a direct lateral approach on the fracture site; together with a partially-threaded screw on the tibial malleolus, with a medial distal approach for the necrotic eschar; as well as a 3.5mm anteroposterior cannulated screw for the posterior malleolus that was placed with a percutaneous approach after reduction with a Verbrugge clamp; and the synthesis was completed with a transsyndesmotic screw supported on the one-third tubular plate of the fibula (Figure 8).
A primary closure of the surgical incision and the pin insertion site was performed, with approximation and closure of the necrotic eschar after debridement with Friedrich-type excision. The patient remained in hospital for 48 hours, with periodic dressing and intravenous antibiotic treatment. On discharge, she continued receiving oral antibiotics and the wound was treated with Aquacel Ag hydrocolloid dressing so that the cellulose fibers combined with silver and disodium salt could absorb the large amounts of exudate and bacteria that came from the wound, and the silver could remove pathogenic microorganisms and prevent biofilm formation. Physical debridement was performed after one week and after 15 days, and finally a granulated area was observed on the site of the necrotic eschar, with complete scar formation after 2 months. We observed a good evolution of all other incisions, and the sutures and staples were removed 20 days after the operation (Figure 9).
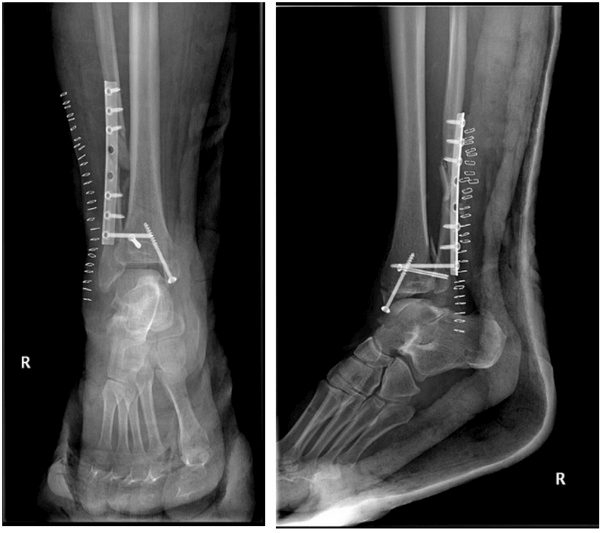
Figure 8: Postoperative RX images.

Figure 9: Wound healing image.
With regard to the involvement of soft tissue, in Case 1 an emergency definitive fixation was performed given the low degree of contamination (Gustilo grade II) and the good condition of the soft tissue on admission. In case 2, the fixation was performed in two stages due to the risk of complications of the soft tissue induced by the severe comminution of the tibial fracture and the causal mechanism. In case 3, a definitive fixation was ruled out at first in the left ankle due to the significant degree of contamination (Gustilo grade III) and the severe involvement of the soft tissue, with edema and blistering skin lesions.
Discussion
The treatment of complex ankle fractures is conditioned by different variables that can lead to a technically difficult management with uncertain results. These variables include the type of lesion and the causal mechanism, the bone quality and the condition of soft tissue [6]. The extension of the soft tissue injury is a direct consequence of the lesion mechanism and the amount of energy that was absorbed at the moment of the trauma [7]. The soft tissue experiences microvascular and inflammatory alterations that cause acidosis and tissue hypoxia, and lead to an initial stage of local inflammation which is associated with increased endothelial permeability and local edema. Afterwards, the inflammation spreads to the surrounding areas, and the lesion reaches its highest level of edema and inflammation after 24-72 hours, which can cause poor scarring and infection, both superficial and deep [8].
There are different classifications for soft tissue injuries associated to fractures, and in this study we have chosen the Tscherne classification, which applies to tibial fractures and is shown in the following (Table 1) [9].
Table 1: Classification of soft tissue damage for closed fractures (Tscherne).
|
Grade |
Diagnosis for soft tissue |
|
Grade 0 |
No injury |
|
Grade 1 |
Contusion from within, superficial abrasion |
|
Grade 2 |
Deep contaminated abrasion, significant abrasion (blistering) and edema with impending compartment syndrome, extensive contusion damage to skin or muscles |
|
Grade 3 |
Skin or muscle necrosis, skin or muscle avulsion, extensive contusion or crushing injury, muscle damage may be severe, vascular injury or compartment syndrome |
One of the main markers that need to be taken into consideration when assessing the grade of a soft tissue injury is inflammation. Therefore, the disappearance of skin folds or of the so-called “wrinkle sign” will suggest moderate to severe inflammation, and paleness or a prolonged capillary refill time will indicate severe edema [8].
The presence of blisters on the skin is a marker for the viability of the tissue. Two categories of blisters can be established, those with serous content, which appear 12 hours after the lesion, and those filled with blood, which appear within the first hours and represent a deeper lesion with a higher risk for poor scarring. The different treatment methods (aspiration, dressing with silver sulfadiazine or leaving them intact) have been compared in the literature, and the prevailing recommendation is leaving them intact except in the case of spontaneous rupture [10]. In order to minimize the injuries in the soft tissue, we shall immobilize the fracture as early as possible, with a previous reduction if necessary, accompanied by the use of cryotherapy techniques, guided compression measures, and a surgical plan in different stages with a minimally invasive approach and low-profile plates [8].
With regard to the lesion mechanism as a factor associated with the evolution of the fractures, these fractures can be divided into two groups: those caused by axial compression and those that result from torsional forces [10, 11]. A rotational lesion generally leads to large metaphyseal fragments with minimal comminution and impaction of the joint and less damage to the soft tissue. On the other hand, fractures resulting from axial compression present severe comminution with impacted fragments, articular cartilage damage and severe involvement of soft tissue [12].
From a historical perspective, when choosing a treatment for these fractures, the first reported series opted universally for open reduction and internal fixation, and the prognostic variables that were associated with the final result were the type of fracture, the quality of the reduction and the method of treatment, with the worst functional results obtained in the more severe fractures, those with a poorer articular reduction and those in which the fixation was least stable [12, 13]. In the decade of the 90s, it was commonly believed that a good condition of the soft tissue was necessary for good results, and Sirkin et al. (1999) and Patterson and Cole (1999) proposed a treatment in two stages [14, 15].
In the year 2000, Watson et al. presented a treatment method based on the condition of the soft tissue, graded according to a classification by Tscherne and Gotzen, regardless of the fracture pattern [9, 16]. Consequently, Tscherne grade 0 and I lesions were treated with open reduction and osteosynthesis, in line with the AO/ASIF guidelines; and in grade II and III lesions, an emergency treatment is indicated with the distraction of the lesion through calcaneal traction or an external fixator accompanied by open reduction and internal osteosynthesis of the fibula. Currently, the use of external fixators is indicated for fractures caused by axial compression and with severe involvement of soft tissue, and a definitive fixation of the fibula combined with external fixation is not indicated because the anatomical reduction of the fibula does not allow contact with fragments in the distal tibial metaphysis, which is associated with a high incidence of delayed consolidation or pseudoarthrosis [17].
With regard to the surgical technique, in definitive surgery procedures it is necessary to use a non-traumatic approach with careful hemostasis, to consider the use of drainage and skin flaps, and to separate the incisions with 7-10cm skin bridges, as well as to use the tourniquet for as short as possible. No primary closure with tension may be applied, so that there can be healing by secondary intention, and it may be necessary to consider the possibility of making releasing incisions [8, 18, 19].
In CIII wounds it is necessary to carry out a debridement of the necrotic tissue in order to prevent superinfection of the site. The first stage in the debridement process involves cleaning the site with abundant liquid (saline, chlorhexidine 0.05% or povidone-iodine 0.5-1%) and removing all the devitalized tissue. The literature reports good results after pressure cleaning and the use of antibiotics with the last cleaning vials. The following debridement techniques are considered: 1) autolytic or physiological debridement with the use of hydrocolloid dressing such as Aquacel dressing; 2) enzymatic or chemical debridement with products based on collagenase (IRUXOL - NOVUXOL - SANTYL), fibrinolysin (PARKELASE) or trypsin (DERTRASE); physical or surgical debridement. The goal is to obtain an adequate granulation tissue, so that a definitive closure can be planned, or healing by secondary intention can be reached [8, 20].
Conclusion
i. Currently, in order to prevent or reduce the complications resulting from the direct surgical treatment of high-energy trauma in the distal end of the tibia, it is essential to properly manage the soft tissue by reducing the devascularization of bone fragments and alternating the use of different techniques of stabilization and indirect reduction, based on the type of lesion (involving the bone, the joint or the soft tissue) and the characteristics of the patient (age, associated pathologies, vascular pathology, tobacco use, etc.) [21].
ii. The moment in which definitive surgery is performed is also an important factor. An operation carried out in the presence of severe intradermal edema or haemorrhagic edemas can increase the risk of tension in the wound, devitalizing the skin and increasing tissue necrosis, with the subsequent development of an infection [7].
iii. Direct internal fixation must not be applied universally. Significant advantages have been described in association with the use of procedures in two stages through the use of external fixation in complex fractures with associated soft tissue injury [10, 18].
iv. In the cases described in our study, the choice of a treatment that is adequate for the fracture pattern, articular lesion and involvement of the soft tissue, and meticulous with regard to articular reconstruction, axial alignment of the limb and management of soft tissue allowed us to obtain satisfactory clinical results and a low incidence of complications, considering the initial severity of the lesions.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Mon 20, Jul 2020Accepted: Wed 05, Aug 2020
Published: Fri 14, Aug 2020
Copyright
© 2023 Montoya Saenz Rocio. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.08.17
Figures & Tables
Table 1: Classification of soft tissue damage for closed fractures (Tscherne).
|
Grade |
Diagnosis for soft tissue |
|
Grade 0 |
No injury |
|
Grade 1 |
Contusion from within, superficial abrasion |
|
Grade 2 |
Deep contaminated abrasion, significant abrasion (blistering) and edema with impending compartment syndrome, extensive contusion damage to skin or muscles |
|
Grade 3 |
Skin or muscle necrosis, skin or muscle avulsion, extensive contusion or crushing injury, muscle damage may be severe, vascular injury or compartment syndrome |
References
- Tim Schepers, Mark R De Vries, Esther M M Van Lieshout, Maarten Van der Elst (2013) The timing of ankle fracture surgery and the effect on infectious complications; A case series and systematic review of the literature. Int Orthop 37: 489-494. [Crossref]
- Rüedi TP, Allgöwer M (1969) Fractures of the lower end of the tibia into the ankle-joint. Injury 1: 92-99.
- M J Patterson, J D Cole (1999) Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Orthop Trauma 13: 85-91. [Crossref]
- Nelson F SooHoo, Lucie Krenek, Michael J Eagan, Barkha Gurbani, Clifford Y Ko et al. (2009) Complication Rates Following Open Reduction and Internal Fixation of Ankle Fractures. J Bone Joint Surg Am 91: 1042-1049. [Crossref]
- P Höiness, L Engebretsen, K Strömsöe (2001) The influence of perioperative soft tissue complications on the clinical outcome in surgically treated ankle fractures. Foot Ankle Int 22: 642-648. [Crossref]
- Rodriguez Castells F Fracturas de pilón tibial. Rev Asoc Arg Ortop y Traumatol 61: 312-321.
- J Borrelli Jr, L Catalano (1999) Open reduction and internal fixation of pilon fractures. J Orthop Trauma 13: 573-582. [Crossref]
- Tull F, Borrelli J (2003) Lesión de partes blandas asociadas a las fracturas cerradas: Valoración y tratamiento. J Am Acad Orthop Surg (Edición Española) 2003: 59-66.
- H Tscherne, H J Oestern (1982) A new classification of soft-tissue damage in open and closed fractures (author's transl). Unfallheilkunde 85: 111-115. [Crossref]
- C P Giordano, K J Koval, J D Zuckerman, P Desai (1994) Fracture blisters. Clin Orthop Relat Res 307: 214-221. [Crossref]
- Elias S Vasiliadis, Theodoros B Grivas, Spyridon A Psarakis, Evangelos Papavasileiou, Angelos Kaspiris et al. (2009) Advantages of the Ilizarov external fixation in the management of intra-articular fractures of the distal tibia. J Orthop Surg Res 4: 35. [Crossref]
- J F Kellam, J P Waddell (1979) Fractures of the distal tibial metaphysis with intra-articular extension—the distal tibial explosion fracture. J Trauma 19: 593-601. [Crossref]
- D N Ovadia, R K Beals (1986) Fractures of the tibial plafond. J Bone Joint Surg Am 68: 543-551. [Crossref]
- M Sirkin, R Sanders, T DiPasquale, D Herscovici Jr (1999) A staged protocol for soft tissue management in the treatment of complex pilon fractures. J Orthop Trauma 13: 78-84. [Crossref]
- M J Patterson, J D Cole (1999) Two-staged delayed open reduction and internal fixation of severe pilon fractures. J Orthop Trauma 13: 85-91. [Crossref]
- J T Watson, B R Moed, D E Karges, K E Cramer (2000) Pilon fractures. Treatment protocol based on severity of soft tissue injury. Clin Orthop Relat Res 375: 78-90. [Crossref]
- T M Williams, J L Marsh, J V Nepola, T A DeCoster, S R Hurwit et al. (1998) External Fixation of Tibial Plafond Fractures: Is Routine Plating of the Fibula Necessary? J Orthop Trauma 12: 16-20. [Crossref]
- D B Thordarso (2000) Complications after treatment of tibial pilon fractures. Prevention and Management strategies. J Am Acad Orthop Surg 8: 253-265. [Crossref]
- B Wyrsch, M A McFerran, M McAndrew, T J Limbird, M C Harper et al. (1996) Operative treatment of fractures of the tibial plafond: A randomized, prospective study. J Bone Joint Surg Am 78: 1646-1657. [Crossref]
- Contreras Ruiz J, Fuentes Suárez A, Arroyo Escalante S, Moncada Barron D, Sosa de Martínez MC et al. (2016) Estudio comparativo de la eficacia de la larvaterapia (LT) para desbridar y controlar la carga bacteriana en úlceras venosas comparado con desbridamiento quirúrgico y aplicación de un antimicrobiano tópico. Gac Méd Méx 152: 78-87.
- Allende C, Bitar I, Cocco CA, Remondino RG, Ortiz N et al. (2001) Fracturas de alta energía del extremo distal de la tibia. Principios de tratamiento y resultados. Rev Asoc Arg Ortop y Traumatol 67: 74-82.