Biliary Colic Presenting as Right-Sided Cervical Radiculopathy
A B S T R A C T
A 50-year-old female patient presented with several weeks of right-sided neck, posterior shoulder, and arm pain suggestive of cervical radiculopathy. Her diagnostic workup included cervical spine x-rays and a cervical spine MRI which showed degenerative changes and mild cervical spinal stenosis. She was evaluated by a spine surgeon and a pain medicine specialist. Multiple treatments were administered without success, including courses of celecoxib and gabapentin. Several rounds of epidural steroid injections were also administered, with only transient relief. Upon developing acute right upper quadrant abdominal pain and undergoing a laparoscopic cholecystectomy for biliary colic, the patient reported resolution of her chronic right neck, posterior shoulder, and arm pain.
Keywords
Atypical manifestation, neck pain, biliary lithiasis, cholecystitis, cholelithiasis, cervical radiculopathy
Introduction
Cervical radiculopathy is a well-documented clinical condition that is caused by compression or irritation of the cervical nerve roots [1]. Patients will typically present with neck pain with or without arm pain which may occur in combination with sensorimotor deficits or diminished reflexes. In the fifth and sixth generation of life, the most common cause of cervical radiculopathy is degeneration of the vertebral discs [2]. A common clinical presentation includes unilateral neck, shoulder, and arm pain. Cervical x-rays and MRI’s may show degenerative changes, central spinal canal stenosis, or neural foraminal stenosis.
Obstruction of the biliary tree can cause biliary colic, cholecystitis, or cholangitis. Risk factors include female gender, obesity, and rapid weight loss. Pain from such an obstruction is typically localized to the right upper quadrant of the abdomen, though may radiate into the back and less commonly to the right scapula. The most common treatment for biliary colic or cholecystitis is elective laparoscopic cholecystectomy.
Case Report
A 50-year-old female obese patient developed right-sided neck pain that radiated to the posterior shoulder and down the right arm in January of 2020. The patient denied any precipitating event. There was no pain in the hand and no upper extremity weakness nor numbness. While the pain was reportedly vague, she did note that it was exacerbated by lying on her right side. The patient denied any other systemic symptoms. The only past medical/surgical history of note was a diagnosis of essential hypertension. Prior to her visit, she had undergone a series of conservative therapies including rest, over the counter and prescription NSAIDs, physical therapy and home exercise regimens, all without relief.
On physical exam, the patient had a positive right-sided Spurling test. The remainder of the neurological and musculoskeletal exam was unremarkable. A diagnosis of right cervical radiculopathy was made. The patient was prescribed short courses of gabapentin and celecoxib, which provided no relief. Cervical spine x-rays showed mild spondylitic changes (Figure 1A). Cervical MRI showed multilevel degeneration and mild stenosis at multiple cervical levels (Figure 1B). An EMG was performed which came back normal.
Between March and June of 2020, 3 rounds of epidural steroid injections were administered which provided transient relief for 1-2 weeks before recurrence of symptoms. A rheumatologic serology panel was ordered and came back negative. An MRI of the right brachial plexus was performed and was normal. A referral to Neurology and subsequent brain MRI did not reveal an alternative diagnosis. Head and neck ultrasound, upper extremity Doppler ultrasound, a thyroid panel, and CT angiography of the neck with contrast all came back unremarkable as well. In November of 2021 the patient developed acute abdominal pain suggestive of biliary colic, which prompted her to undergo an elective laparoscopic cholecystectomy. Her post-operative course was uncomplicated, and upon follow-up for her neck and arm pain approximately 3 weeks later, the patient reported nearly complete resolution of her symptoms.
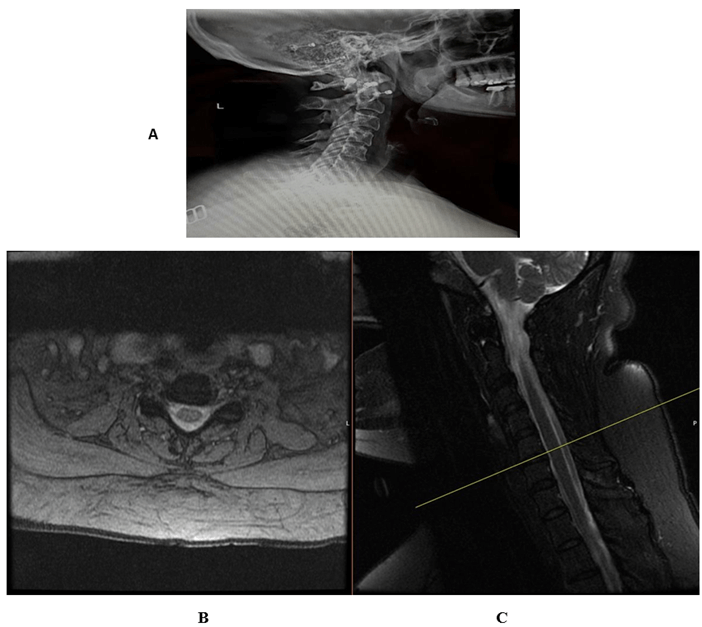
Figure 1: A) (Above) lateral Xray of cervical spine 6/1/21, Dynamic instability at C2-C3, C3-C4 and C4-C5 with development of 2 to 3 mm of anterolisthesis with flexion. Findings are most severe at C2-C3. No fracture. Disc space heights are maintained. B) (Below): MRI of the cervical spine 2/9/21 showing multilevel degenerative spondylitic changes; mild stenosis at C5-6 and C3-4.
Discussion
This is a case of a patient with symptoms that mimicked cervical radiculopathy including unilateral neck, shoulder and arm pain, but that resolved after a laparoscopic cholecystectomy. One such sign that further supported the diagnosis was the presence of a positive Spurling test, which manipulates the head in extension and rotation to compress the foramina and elicit a positive pain response [2]. In contrast, biliary colic is usually characterized as waxing and waning postprandial pain mostly located in the right upper quadrant of the abdomen with radiation to the back in some cases [3]. While there have been documented cases of biliary colic pain radiating to the back and even to the right shoulder, the course of this patient’s pain beginning from the neck and radiating down to the medial aspect of the wrist is unique from other documented cases of referred pain from biliary colic.
Article Info
Article Type
Case ReportPublication history
Received: Mon 20, Jun 2022Accepted: Mon 25, Jul 2022
Published: Fri 19, Aug 2022
Copyright
© 2023 Alexander Kervyn De Volkaersbeke. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2022.08.03
Figures & Tables
References
1. Iyer S, Kim HJ (2016) Cervical
radiculopathy. Curr Rev Musculoskelet Med 9: 272-280. [Crossref]
2. Magnus W, Viswanath O, Viswanathan VK (2022) Cervical Radiculopathy. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. [Crossref]
3. Sigmon DF, Dayal N, Meseeha M (2022) Biliary Colic. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. [Crossref]