Journals
Atypical Presentation for Colorectal Cancer
A B S T R A C T
Bowel cancer is the second most common non-cutaneous cancer diagnosed in Australia in both the sexes. Australia has one of the highest incidence of bowel cancer in the world. Pyogenic liver abscess has been reported to be associated with malignancy especially hepatobiliary and colorectal cancer.
A healthy 70 years old woman presented with non-specific symptoms which was initially thought to be secondary to haematological malignancy. Further investigation noted multiple large cystic and solid hepatic masses, which were suggestive of metastasis. However, hepatic lesions responded significantly with antibiotics which was in keeping with liver abscess instead. She was subsequently confirmed to have caecal adenocarcinoma with no distant metastasis.
Although uncommon, pyogenic liver abscess can be the first presentation for colorectal malignancy. Colonoscopy is essential especially if no clear cause of liver abscess is identified.
Keywords
Liver abscess,colorectal cancer,colonoscopy
Introduction
Bowel cancer is the second most common non-cutaneous cancer diagnosed in Australia in both the sexes. Australia has one of the highest incidence of bowel cancer in the world [1]. By the age of 85 years old, the risk of colorectal cancer is one in 11 for male and one in 16 for female [1]. Early detection is essential as localised diseases have five-year relative survival of 89.9% compared to merely 13.8% for patients with distant metastasis [2]. Pyogenic liver abscess has been associated with higher risk of colorectal malignancy.
Case Report
A healthy 70 year old lady presented to the emergency department with one week history of malaise and diarrhea. She denied having fever, abdominal pain, weight loss and per rectal bleeding. Her past medical history was unremarkable. On examination, her abdomen was soft, nontender with hepatomegaly. She did not have any palpable cervical, axillary, subclavian and inguinal lymph nodes. Investigations revealed Hb 65g/L, WBC 47.0 x109/L, PLT 342 x109/L, CRP 296 mg/L. Severe iron deficiency was detected as well.
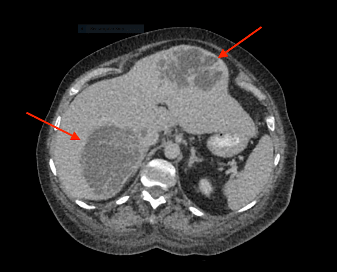
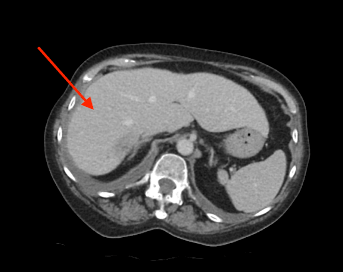
Patient was initially admitted under the medical team for management of likely haematological malignancy with symptomatic anaemia. On further investigation, CT abdomen demonstrated multicystic and solid hepatic masses suggestive of metastasis, but no primary malignancy detected (See figure 1). Findings were further confirmed with ultrasound liver.
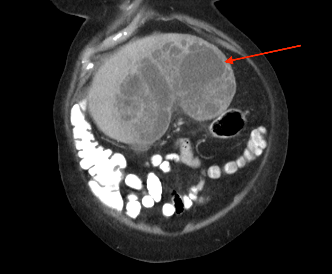
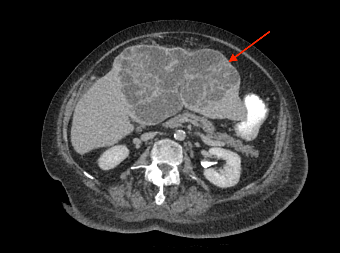
Patient had a complicated in-hospital stay which was further complicated by septic shock secondary to hospital acquired pneumonia and pericardial effusion. A repeat ultrasound liver three weeks later demonstrated a decrease in the size of the liver lesions, suggested that they favour abscess rather than metastasis. Repeat CT abdomen again confirmed the findings and also noted lobulated mucosal thickening at ileocaecal junction, suggestive of colonic neoplasm. Caecal mass was also identified in the initial CT retrospectively, which was missed initially. Colonoscopy confirmed a non-obstructing, non-circumferential mass in the caecum. Histology showed adenocarcinoma. Her liver abscess completely resolved with long course intravenous antibiotics. CT staging did not show any evidence of distant metastasis (See figure 2). An elective uncomplicated laparoscopic right hemicolectomy was performed, and she was subsequently discharged home well day six post op. Histology returned to show pT2N0M0 adenocarcinoma.
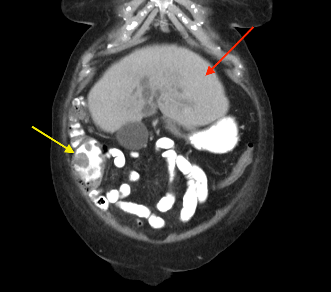
Figure 1 (a, b, c): CT Abdomen showed multicystic and solid hepatic masses. Differential diagnosis includes hydatid cyst, metastasis or abscess.
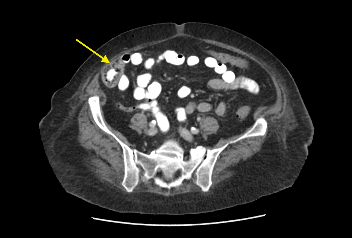
Figure 2: (a, b) Red arrow - Interval CT 2 months later illustrated significant reduction in liver mass in keeping with resolving abscesses. (b, c) Yellow arrow - Large polypoid lesion within the caecum at the ileocaecal region in keeping with carcinoma
Discussion
Clinical features of colorectal cancer may vary significantly depending on the anatomical site and disease stage of the tumour. Early stage disease may not have any symptoms. The most commonly reported symptoms include altered bowel habit, per rectal bleeding, abdominal pain, tenesmus and anaemia [3, 4]. Advanced disease may present with intestinal obstruction or perforation. However, atypical presentations for colorectal cancer have been reported. It is essential for clinicians to recognise them early to improve patient’s outcome. Pyogenic liver abscess has been reported to be associated with increased risk of malignancy especially hepatobiliary cancer and colorectal cancer [5-7].
Risk of colorectal cancer in patients with pyogenic liver abscess is significantly higher with standardised incidence ratio (SIR) of 5.27 (95% CI, 3.76 – 7.18) [5]. It is also more common in male and patients aged <60 [8]. It is hypothesized that breached in colonic mucosal and bacterial translocation are the pathogenesis for liver abscess in colorectal cancer [8]. Klebsiella pneumoniae is found to be the most common pathogen and diabetes mellitus is a known risk factor [6, 8]. Moreover, pyogenic liver abscess with underlying malignancy is associated with higher mortality as compared to non-malignant disease [9]. Imaging-guided percutaneous drainage has been recommended as treatment of choice instead of surgical drainage or antibiotics alone [9]. Nevertheless, our patient had significant improvement on just antibiotics alone.
To conclude, although uncommon, pyogenic liver abscess can be the first presentation for patients with occult colorectal cancer. “The eyes do not see what the mind does not know”. It is essential for clinicians to be aware of the possibility. Colonoscopy is warranted for these patients especially if no clear cause of liver abscess is identified.
Acknowledgements
No potential conflict of interest relevant to this article was reported. All authors have approved the submission.
Article Info
Article Type
Case ReportPublication history
Received: Tue 09, Jul 2019Accepted: Fri 26, Jul 2019
Published: Fri 02, Aug 2019
Copyright
© 2023 Wen Jye Wong. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2019.04.05
Author Info
Corresponding Author
Wen Jye WongDepartment of General Surgery, Bundaberg Hospital, Bundaberg 4670, Queensland, Associate Lecturer, University of Queensland, Australia
Figures & Tables
References
- Cancer Council Australia Colorectal Cancer Guidelines Working Party (2019) Clinical practice guidelines for the prevention, early detection and management of colorectal cancer. Sydney: Cancer Council Australia.
- Noone AM, Howlader N, Krapcho M, Miller D, Brest A et al. (2018) SEER Cancer Statistics Review (CSR)1975-2015. National Cancer Institute, Bethesda.
- Smith D, Ballal M, Hodder R, Soin G, Selvachandran SN et al. (2006) Symptomatic presentation of early colorectal cancer. Ann R Coll Surg Engl 88: 185-190. [Crossref]
- Hamilton W, Round A, Sharp D, Peters TJ (2005) Clinical features of colorectal cancer before diagnosis: a population-based case-control study. Br J Cancer 93: 399-405. [Crossref]
- Kao WY, Hwang CY, Chang YT, Su CW, Hou MC et al. (2012) Cancer risk in patients with pyogenic liver abscess: a nationwide cohort study. Aliment Pharmacol Ther 36: 467-476. [Crossref]
- Jeong SW, Jang JY, Lee TH, Kim HG, Hong SW et al, (2012) Cryptogenic pyogenic liver abscess as the herald of colon cancer. J Gastroenterol Hepatol 27: 248-255. [Crossref]
- Lai HC, Lin HC (2010) Cryptogenic pyogenic liver abscess as a sign of colorectal cancer: a population‐based 5‐year follow‐up study. Liver Int 30: 1387-1393. [Crossref]
- Qu K, Liu C, Wang ZX, Tian F, Wei JC et al. (2012) Pyogenic liver abscesses associated with nonmetastatic colorectal cancers: an increasing problem in Eastern Asia. World J Gastroenterol 18: 2948-2955. [Crossref]
- Yeh TS, Jan YY, Jeng LB, Hwang TL, Chao TC et al. (1998) Pyogenic Liver Abscesses in Patients with Malignant Disease: A Report of 52 Cases Treated at a Single Institution. Arch Surg 1998;133: 242-245. [Crossref]