Atrial Myxoma with Glandular Differentiation – A Case Report
A B S T R A C T
Benign cardiac myxoma with glandular differentiation is an extremely rare subtype of cardiac tumors which can mimic myxosarcoma grossly and histologically. Primary cardiac tumors are extremely rare and account for less than 0.2% of all tumors. They are benign in 75% of cases and almost 50% of these are myxomas. The differentiation between benign and malignant cardiac tumors is challenging by echocardiography or histologically. We report a case of primary left atrial benign cardiac myxoma mimicking myxosarcoma grossly and histologically by its glandular differentiation. Only 39 such cases reported in the literature.
Keywords
Cardiac tumors, myxoma
Introduction
Heart tumors were first recognized by Columbus in 1559. Primary cardiac tumors are extremely rare and account for less than 0.2% of all tumors. They are benign in 75% of cases and about 50% of these are myxomas. Upto 75% of myxomas arise in the left atrium, while 20% arise in the right atrium, and 8% arise in the ventricles [1]. They are believed to arise from remnants of subendocardial vasoformative reserve cells or multipotential primitive mesenchymal cells in the fossa ovalis [2]. Although echocardiography is the primary modality of diagnosis, it is not beneficial in the differentiation between benign and malignant tumor. Furthermore, it is also challenging to distinguish between a cardiac myxoma and myxosarcoma histologically due to their great similarities. In this paper, we report a rare case of primary left atrial benign cardiac myxoma mimicking myxosarcoma grossly and histologically.
Case Report
A 44-year-old male presented with 2-month history of progressively increasing shortness of breath. He was diagnosed to have a left atrial mass in an outside facility and was referred to our center for management. On examination, the patient was anxious but relatively comfortable at rest. Cardiovascular examination revealed a soft first heart sound with typical plopping sound in the mitral area accompanied by a mid-diastolic murmur changing in character and intensity with change in patient posture. A transthoracic echocardiogram revealed a huge mass attached to the inter-atrial septum (Figure 1). The mass was 7.8 cm2 in size. It had a broad stalk, freely mobile, & protruded into the left ventricle during ventricular diastole, almost completely occluding the mitral valve (Figure 2). The left atrium dimension was measured to be 3.4cm2. The mitral valve appeared to have a normal morphology and function. The left and right ventricles had normal systolic and diastolic functions. A pre-operative coronary angiogram was done, which showed no coronary artery disease. The left atrial mass was excised en-bloc with a wide margin of the atrial septum around the stalk. The resultant atrial-septal defect (ASD) was closed with an equine pericardial patch. (Figure 3, 4) The resected mass grossly appeared glandular and jelly like. Histologically, initially was suspected to be myxosarcoma. Upon careful examination and immune-histochemical staining, it was confirmed to be a benign cardiac myxoma with glandular differentiation. An intra operative transesophageal echocardiogram showed no residue myxoma and a normally functioning mitral valve (Figure 5,6). A post-operative Pan CT scan to screen for secondary or metastatic tumors was negative. The patient had a smooth recovery and was discharged home on the fourth post-operative day.
Discussion
Patients with primary cardiac tumors benign or malignant may present with the same clinical features. Symptoms are caused by three main mechanisms: intracardiac obstruction, systemic embolization of tumor fragments, or constitutional symptoms by unclear mechanisms. Primary symptoms include dyspnea, most common presenting symptom (42%), followed by chest pain (7%), and pain & paraesthesia of the limbs (5%) [1]. Echocardiogram is an extremely important tool in diagnosing intra cardiac masses. Furthermore, it is nearly impossible to differentiate between myxomas and myxosarcomas by imaging. Both myxomas and myxosarcomas are characterized by extracellular deposition of proteoglycans and usually are located in the left atrium, which adds to the difficulty in distinguishing between them.
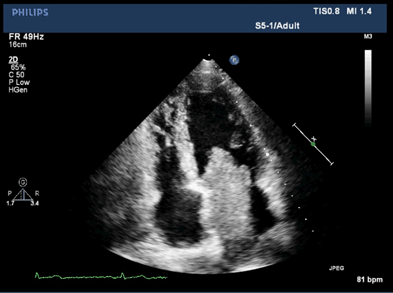
Figure 1: Transthoracic echocardiogram, Apical 4 chamber view, showing a large mass occupying the left atrium.
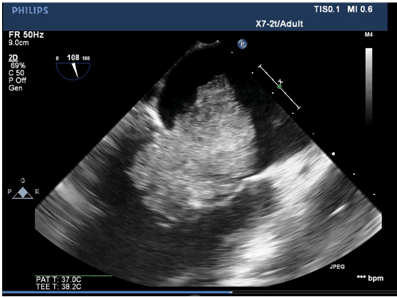
Figure 2: Transthoracic echocardiogram, showing the mass occluding the mitral valve causing servere funcation stenosis.
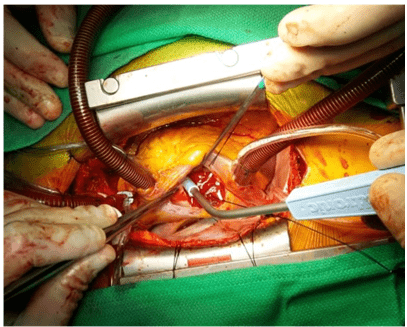
Figure 3: Opening in the right atrium with myxoma attached to the interatrial septum.
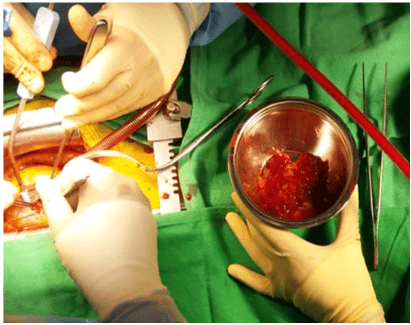
Figure 4: Gross appearance of the gelatinous myxoma on being excised from the left atrial opening.
The most important histological criterion to establish the diagnosis of myxosarcoma is the absence of the typical cords, rings & capillary structures formed by myxoma cells [3]. Therefore, further assessment of the histological manifestation is always required. In our patient, the microscopic examination of the section revealed a benign neoplasm composed of epithelial elements forming cords, nests, rings and glands embedded in myxoid background. Also, focal areas of hemorrhage were seen. Therefore, a diagnosis of left atrial myxoma with glandular differentiation was made. This is an extremely rare subtype with only 39 cases reported in the literature [4]. It is important to distinguish between myxomas and myxosarcomas because of their great differences in patient prognosis. Myxosarcomas have a poor prognosis with a mean survival of about 12 months after diagnosis. Resection is possible only in 50% of cases and the most common cause of death is local recurrence which cannot be prevented by radiation or chemotherapy [5]. Recurrence in myxomas mostly occurs in patient with a positive family history [6].
Conclusion
As cardiac myxomas with glandular differentiation are rare, there is minimal available data regarding its prognosis. Hence, long-term follow up and serial echocardiogram evaluation is necessary.
Article Info
Article Type
Case ReportPublication history
Received: Mon 08, Apr 2019Accepted: Mon 29, Apr 2019
Published: Fri 31, May 2019
Copyright
© 2023 Fayaz aahmed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2019.03.01
Figures & Tables
References
- Nehaj F, Sokol J, Mokan M, Jankovicova V, Kovar F et al. (2018) Outcomes of Patients with Newly Diagnosed Cardiac Myxoma: A Retrospective Multicentric Study. Biomed Rese Int 2018: 8320793. [Crossref]
- Zhang T, Koide N, Wada Y, Tsukioka K, Takayama K et al. (2003) Significance of monocyte chemotactic protein-1 and thymidine phosphorylase in angiogenesis of human cardiac myxoma. Circ J 67: 54-60. [Crossref]
- Diganta Kakaty, Martin Grapow, Bettina Huber, Didier Lardinois. (2015) Long-term survival after extended resection of primary atrial myxosarcoma. J Surg Case Rep 2015: rju146-rju146. [Crossref]
- K.C. B, Karki S (2017) Cardiac myxoma with glandular elements: A case report. Journal of Pathology of Nepal 7: 1224.
- Awamleh P, Alberca MT, Gamallo C, Enrech S, Sarraj A (2007) Left atrium myxosarcoma: an exceptional cardiac malignant primary tumor. Clin Cardiol 30: 306-308. [Crossref]
- Ronny Cohen, Gagandeep Singh, Derrick Mena, Christine A. Garcia, Pablo Loarte et al. (2012) Atrial Myxoma: A Case Presentation and Review. Cardiol Res. 3: 41-44. [Crossref]