Journals
An air powered gunshot wound to the chest, pellet missing with a trace
Case Report
A 55-year-old male arrived at our emergency department 60 minutes after being shot by an air powered rifle in the right chest. Immediately after the incident he was in respiratory distress, although his clinical condition improved following a bout of productive haemoptysis. During first examination he was alert but stubbornly, peripheral oxygen saturation of 96% with 12 litres of oxygen, blood pressure 109/75 mmHg, and a sinus rhythm of 100 bpm. Above the right nipple next to the right edge of the sternum a penetrating entrance wound was indentified. There was no sign of an exit wound. Auscultation revealed diminished breath sounds in the right chest. Ultrasound showed dorsal and basal pleural effusion in the right chest. The patient’s clinical condition remained stable; a chest X-ray and a CT scan were performed [1, 2].
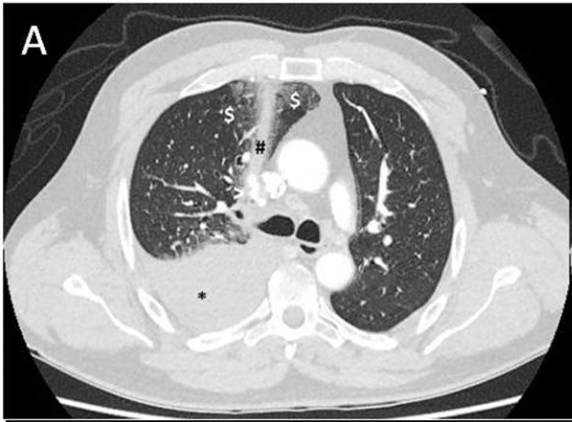
A right hemothorax (X-ray not shown) was most likely caused by damage to the right pulmonary artery with the trajectory of the pellet passing in close proximity to the aorta (figure 1A) and affecting the anterior wall of the right main bronchus only (Figure 1B). A chest drain insertion was attempted under local anaesthesia but unsuccessful due to lack of patient’s cooperation. After a multidisciplinary deliberation the decision was made to give the patient general anaesthesia, drain the hemothorax and perform a selective angiogram. 700 mL of blood was drained immediately. Angiography identified an active bleeding point from the right pulmonary artery. This was successfully coiled (figure 1C and D). At the end of this procedure the total amount of blood drained was 950 mL. Trauma to the right main bronchus was bronchoscopically inspected. A small lesion (< 6mm) was seen on the anterior wall of the right main bronchus without an active bleed and only minimal swelling. A clinically stable patient, the lack of air leakage from the chest tube, subcutaneous emphysema or pneumothorax under positive pressure ventilation and no evidence of oesophageal injury made us classify this injury as a small without airway compromise. Non-surgical, conservative treatment was chosen in this traumatic penetrating injury. The patient was extubated at the end of the bronchoscopic procedure. Nevertheless, the pellet was still missing. CT scan analysis suggested a pellet exit via the right main bronchus. The pellet was found at the scene of the shooting within a coughed-up blood clot (Figure 1E). The postoperative and recovery period were uneventful.
Penetrating tracheobronchial injury in trauma is rare. Although the exact incidence is unknown as many of these patients die in the pre-hospital period it is estimated as < 1-2% [1]. After initial assessment of the airway, surgical repair is the cornerstone for large airway defects especially in the presence of major clinical symptoms as oesophageal injury, progressive emphysema, severe dyspnoea, difficult mechanical ventilation and massive air leakage [2, 3]. To restore anatomical integrity, adequate imaging is essential [4, 5]. Conservative non-operative management can be used when criteria suggested by Ross are met [6]. Initially suggested for post intubation injury it is seldom used for trauma induced injuries because major clinical symptoms are often present.2 At first only minor defects (< 2 cm) were treated conservatively using Ross criteria, nowadays larger injuries are successfully managed without surgery [1, 2, 5]. This report shows that conservative treatment using Ross criteria is also possible in penetrating tracheobronchial injury caused by an air powered gunshot wound in the absence of major clinical symptoms.



Conflict of Interests
All authors declare no conflict of interest.
Funding
No financial support
Authors Contribution
All authors have participated in constructing the article, all have read the final submission.
Article Info
Article Type
Case ReportArticle History
Received: 19 October, 2018Accepted: 12 November, 2018
Published: 3 December 2018
Copyright
© 2018 Cornelis Slagt. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.10.31487/j.SCR.2018.03.017
Author Info
Corresponding author
Cornelis SlagtRadboud University Medical Centre, Department of Anaesthesiology, Pain and Palliative Care, Geert Grooteplein Zuid 10, 6500 HB Nijmegen, The Netherlands.
Figures & Tables
References
1. Prokakis C, Koletsis EN, Dedeilias P, Fligou F, Filos K, et al. (2014) Airway trauma: a review on epidemiology, mechanisms of injury, diagnosis and treatment. J Cardiothorac Surg. 9: 117. [Crossref]
2. Gómez-Caro A, Ausín P, Moradiellos FJ, Díaz-Hellín V, Larrú E, et al. (2006) Role of conservative medical management of tracheobronchial injuries. J Trauma 61: 1426-1434. [Crossref]
3. Wandling MW, Hoel AW, Meyerson SL, Rodriguez HE, Shapiro MB, et al. (2015) Complex Intrathoracic Tracheal Injury. Am J Respir Crit Care Med 192: e20-21. [Crossref]
4. Ro T, Murray R, Galvan D, Nazim MH (2015) Atypical gunshot wound: Bullet trajectory analyzed by computed tomography. Int J Surg Case Rep 14: 104-107. [Crossref]
5. Kovacs G, Sowers, N (2018) Airway Management in Trauma. Emerg Med Clin North Am 36: 61-84. [Crossref]
6. Ross HM, Grant FJ, Wilson RS, Burt ME (1997) Nonoperative management of tracheal laceration during endotracheal intubation. Ann Thorac Surg 63: 240-242. [Crossref]