An Affordable and Universal Treatment for ‘Barcode’ Upper Lip Wrinkles
A B S T R A C T
A study was conducted to assess the cost-benefit ratio of manual dermabrasion with an electrocautery scratch pad for upper lip wrinkles. The study included 15 patients with a follow-up ranging from 4 to 108 months. The post-operative course was uneventful without serious complications and all patients were pleased with the results. The mean healing time was 10 to 15 days. The procedure can be performed safely for out-patients with a mean operative time of 30 minutes. The medical supply for the procedure is easily available worldwide and the cost does not exceed 20 euros per patient. It is also a versatile technique that can be performed under local anaesthesia by a surgeon trained with facial nerve blocks. The only drawback is the social exile during the healing time.
Keywords
Lip, Wrinkles, dermabrasion
Introduction
Because lips are a very dynamic organ and are the first tissues exposed to toxic and environmental factors such as tobacco and sun damage, development of upper lip wrinkles is a frequent concern of women who want to retrieve a youthful appearance. The usual presentation of these wrinkles is vertical lines giving the appearance nicknamed barcode lines. The density and the depth of these wrinkles are highly variable among patients related to genetic conditions but tend to increase with age and are very disturbing as they occur more frequently in women [1]. A wide range of procedures have been proposed to treat this condition from minimally invasive procedures to high-tech techniques but no critical analysis has been engaged about the cost of these treatments although it is crucial in these times of financial restriction. For these reasons, we have undertaken a retrospective observational study on simple mechanical dermabrasion to determine the cost-benefit ratio of this procedure.
Materials and Methods
I Materials
15 patients were enrolled in the study. All patients were female. All patients were Caucasian. The age ranged from 46 to 74 years (mean age: 63.6 years). All patients signed an informed consent. One patient receiving an anticoagulant treatment (clopidogrel, Plavix®) was included in the study because she already had a major aesthetic surgery (face lifting) without any complications. One patient had an iterative dermabrasion 9 years after the initial procedure. Six patients were operated on under general anaesthesia undertaken for a complementary aesthetic procedure, while the other patients were operated on under local anaesthesia achieved by a bilateral infraorbital nerve block completed at the anterior nasal spine with a 1% articaine solution (Ubistesin®,3M France, Cergy-Pontoise). The anaesthesia was effective after 5 to 10 minutes and the dermabrasion of the white lip was done with a presterilized cautery scratch pad (FIAB, Via Costoli, 4, Florence, Italy). After pinching the lips, the dermabrasion was performed with the folded pad by gentle pressure and stopped when a uniform bleeding of the skin was observed. A swab moist with a 3% hydrogen peroxide solution was applied until bleeding stopped completely. An antiseptic ointment (Biafine®, Johnson & Johnson, France) was then applied on the scar twice a day until the last scab had fallen.
II Methods
A photographic chart was established with a standardized view including the nose and chin for references. The results were assessed by the single investigator. Feedback was obtained from the patients by photos from smartphones if they noticed any problem. A postoperative appointment was given between 10 and 30 days later and then the follow up ranged between 4 and 108 months with a mean follow-up time of 27,7 months). The aesthetic results were assessed with clinical observation of the skin (mainly the pigmentation) and a semi-quantitative method based on the number and depth of the wrinkles on pre and post treatment photographs. It was categorized as grade 0 with no results or definitive complications, grade 1 for partial improvement with reduction of the depth or number of the wrinkles and grade 2 for complete improvement of both depth and number of the wrinkles.
Results
The surgery could be achieved without any problems in all patients under local anaesthesia. No prolonged post-operative bleeding was observed after 15 to 20 minutes. The patient treated with clopidogrel did not stop taking her treatment and had a normal bleeding. One patient was worried about a possible local infection at day 7 but no general antibiotic was prescribed and the healing was uneventful with a topical treatment alone.
All patients were satisfied with the results. The surgery was completely painless with local anaesthesia and postoperative pain was easily controlled with usual medication. It was difficult to determine the exact mean healing delay but all patients who had an appointment after day 60 healed completely at this time without any scabs. In most patients, we observed a mild erythema during a few weeks and then the lip retrieved a normal pigmentation. There was no postoperative sensory disturbance. At 4 months, all patients had an improvement and 14 (87.5%) displayed a grade 1 result (Figures 1-3) and 2 (12.5%) a grade 2 result (Figures 4-6). Patients with a follow-up of more than one year showed some degree of recurrence. The patient with the longer follow-up returned to her original condition and agreed to have a new procedure with good immediate results.
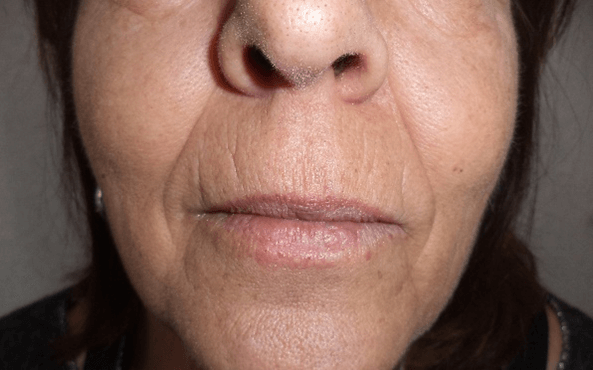
Figure 1: Pre-operative view of a patient graded 1.

Figure 2: Result at day 7 showing residual scabs.

Figure 3: Result after 18 months.

Figure 4: Pre-operative view of a patient graded 2.

Figure 5: Result at day 17 showing mild erythema.

Figure 6: Result after 5 months.
Discussion
Microdermabrasion remains one of the most frequent non-invasive procedures (700000 procedures performed in 2017 according to the statistical report of the American Association of Plastic Surgeons). It has been suggested in the literature that it was first used by the ancient Egyptians using sandpaper. In more recent times there were several attempts to improve the procedure with a motorized device. The main problem by using rotative instruments is that it is very difficult to control exactly the depth of the dermabrasion [2]. It might also be dangerous because this technique causes the diffusion of microparticles with possible risk of disease transmission for the surgeon and assistants. For these reasons, sandpaper has been advantageously replaced by electrocautery scratch pads that are commonly available in every operating room [3]. Among alternative minimally invasive procedures, fillers have received more recent attention for facial rejuvenation [4]. In our experience, fillers are not suitable for these fine wrinkles because several patients complained of noticeable contour irregularities. Another main drawback is that fillers have no long lasting effects. Another non- invasive technique has been introduced more recently with emulsified fat injection [5]. The main limitation of this technique is the additional procedure and the fat resorption regularly reported with lipofilling techniques. The most studied invasive treatment for perioral wrinkles is ablative carbon dioxide laser.
Although this technique has been shown to be effective for skin resurfacing, it does not offer a clear advantage over manual dermabrasion in comparative studies [6, 7]. The main concern in all these techniques remains the cost issue. In our study, the cost of an electrocautery scratch pad is less than one euro and the general furniture (anaesthetic solution, syringe, swabs) does not exceed 20 euros per patient so the cost-benefit ratio is unbeatable. Considering the risk-benefit ratio, the aesthetic results were also very good with manual dermabrasion producing an improvement in all cases although the patients with the longest follow-up showed a recurrence of the wrinkles. The main concern of dermabrasion is the risk of postoperative definitive dyschromia. All patients in our study experienced a short term erythema lasting for a few weeks, but no one complained of definite postoperative depigmentation. Other clinical studies demonstrate that this complication is unusual [8, 9].
However, because of severe legal regulations in aesthetic medicine and surgery we recommend is to be very careful with patients with pigmented skin and to focus on this risk with all patients. This technique is also very safe and the bleeding can be easily controlled with a hydrogen peroxide sponge [10]. The patient at risk of bleeding in our study did not stop her treatment, but we recommend to discontinue the platelet inhibitor medication a few days the procedure before if it is possible. The risk of postoperative infections must also be taken into consideration, but we do not recommend a postoperative systemic antibiotic treatment that can be deleterious by causing microbial resistance. A preoperative treatment with an antiviral treatment can be proposed to prevent a herpes outbreak in patients with a history of this disease. The only disappointment we met in our study were the limited results for deep wrinkles so it advisable not to have unrealistic hopes in these cases.
Conclusion
Our study demonstrates that dermabrasion is an affordable and safe procedure and should be considered in the first instance for upper lip wrinkle treatment. Results on superficial fine lines are particularly dramatic but expectation for deep wrinkles must be more reasonable. It can be performed easily at an office surgery with light postoperative care and it is not very painful. It can also be repeated after a few years. The only potential adverse effect is postoperative dyschromia and thus it should be considered carefully in patients with pigmented skins. Finally, the only unavoidable inconvenience for the diffusion of this technique is the social exile that last in most of cases for less than ten days. In the future, the technique may also be advantageously extended to other areas of the face, more particularly the nose and the periorbital region [11, 12].
Conflicts of Interest
None.
Article Info
Article Type
Research ArticlePublication history
Received: Sat 13, Feb 2021Accepted: Thu 25, Feb 2021
Published: Thu 11, Mar 2021
Copyright
© 2023 L. DUPOIRIEUX. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.03.09
Figures & Tables
References
1. Paes EC, Teepen HJLJM, Koop WA, Kon M (2009) Perioral wrinkles : Histologic differences between men and women. Aesthet Surg J 29: 467-472. [Crossref]
2. Smith B, Conway S (1979) A new technique of dermabrasion. Ann Plast Surg 3: 149-150. [Crossref]
3. Kidwell MJ, Arpey CJ, Messingham MJ (2008) A comparison of histologic effectiveness and ultrastructural properties of the electrocautery scratch pad to sandpaper for manual dermabrasion. Dermatol Surg 34: 1194-1199. [Crossref]
4. Chiu A, Fabi S, Dayan S, Nogueira A et al. (2016) Lip injection techniques using small-particles hyaluronic acid dermal filler. J Drugs Dermatol 15: 1076-1082. [Crossref]
5. Mesguich Batel F, Bertrand B, Magalon J, François P, Velier M et al. (2018) Treatment of wrinkles of the upper lip by emulsified fat or "Nanofat": Biological and clinical study about 4 cases. Ann Chir Plast Esthet 63: 31-40. [Crossref]
6. Gin I, Chew J, Rau KA, Amos DB, Bridenstine JB (1999) Treatment of upper lip wrinkles: a comparison of the 950 microsec dwell time carbon dioxide laser to manual tumescent dermabrasion. Dermatol Surg 25: 468-473. [Crossref]
7. Holmkvist KA, Rogers GS (2000) Treatment of perioral rhytides: a comparison of dermabrasion and superpulsed carbon dioxide laser. Arch Dermatol 136: 725-731. [Crossref]
8. Ship AG, Weiss PR (1985) Pigmentation after dermabrasion: an avoidable complication. Plast Reconstr Surg 75: 528-532. [Crossref]
9. Weisman O, Zilinsky I, Farber N, Ben-noon HI, Stavrou D et al. (2012) A new simple, safe, and easy solution for upper lip dermabrasion. J Drugs Dermatol 11: 649-652. [Crossref]
10. Weiss J, Winkelman FJ, Titone A, Weiss E (2010) Evaluation of hydrogen peroxide as an intraprocedural hemostatic agent in manuel dermabrasion. Dermatol Surg 36: 1601-1603. [Crossref]
11. Emsen IM (2008) A different and cheap method: sandpaper (manual dermasanding) in treatment of perirorbital wrinkles. J Craniofac Surg 19: 812-816. [Crossref]
12. Chuang GS, Alfaresi F (2018) Regional dermabrasion of nasal surgical scars and rhinophyma using electrocautery scratch pads. Dermatol Surg 44: 300-302. [Crossref]