Acute Adult Jejuno-Jejunal Intussusception Caused by a Giant Lipoma
A B S T R A C T
Acute abdominal pain secondary to intussusception is rare in adults and mainly caused by malignancy (70-90%), whereas in childhood intussusception’s etiology is mostly idiopathic (90% of cases). Gastrointestinal lipomas, especially in small bowel, represent an unusual cause of intussusception with complete intestinal obstruction or bleeding (acute or chronic) from mucosal ulceration. In acute settings, computed tomography (CT) should be confidently considered the gold standard for diagnosis. In adulthood, surgical management of acute symptomatic intussusception caused by lipoma is mandatory. We report a case of complete jejunal obstruction with intussusception due to 5 cm submucosal lipoma.
Keywords
Intussusception, small bowel, obstruction, lipoma, computed tomography, acute abdomen
Introduction
Gastrointestinal lipomas in adults are rare benign diseases, representing only 1-2% of gastrointestinal neoplasm [1]. The majority of small bowel lipomas are solitary [2]. The most common site of growth is in the colon, followed by small bowel, rarely they present in the stomach [3]. Small lesions are frequently asymptomatic, but bigger lesions (more than 2 cm) may present history of abdominal bloating and/or chronic abdominal pain or can lead to an acute clinical presentation such as intussusception or bleeding [4]. We described a case of jejuno-jejunal intussusception due to submucosal lipoma.
Case Report
An 80-year-old female with a history of hypertension and previous open surgery appendectomy in childhood, was admitted to our emergency department complaining of acute abdominal pain lasting two days. The patient had no recent history of alteration in bowel habits, melena, or weight loss. Physical examination revealed abdominal tenderness and distension with localized peritoneal signs. No palpable abdominal masses were appreciated. Plain abdominal radiography showed significant gastric dilatation with air-fluid level.
A contrast-enhanced computed tomography (CT) of the abdomen was performed, which demonstrated a suspected jejunal intussusception (target sign) due to fatty density homogenous mass measuring 5 cm that was recognized to be the lead-point of the invagination and suspected of lipoma (Figure 1). No pneumoperitoneum was detected. The patient was admitted to the surgical department, fluids were infused, and a nasogastric tube was placed. An emergency laparotomy was performed and, 30 cm distally to Treitz ligament, a jejuno-jejunal intussusception was found (Figure 2). According to benign CT findings, we conducted a partial reduction of intussusception. The presence of soft intramural palpable mass and irreversible ischaemia in a small part of the invaginated bowel, lead us to mandatory small bowel segmental resection and primary side-to-side anastomosis. Gross examination of the specimen revealed a submucosal ovalar tumor of 5 cm on the maximum axis. Histopathological analysis confirmed the diagnosis of submucosal lipoma with no signs of dysplasia or malignancy. A small bowel follow-through was ordered on day sixth: no leakage occurred, and the water-soluble contrast medium progression was regular. The postoperative recovery period was uneventful, and the patient was discharged on day nine.

Figure 1: Contrast-enhanced CT scans. Axial cut view showing A) intussusception as a sausage-shaped lesion (arrows) and C) target-shaped lesion (arrowheads). Sagittal cut view B) shows the lead point of intussusception, compatible with lipoma (star).
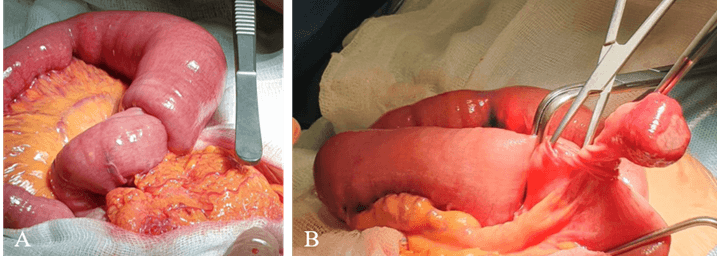
Figure 2: Intraoperative findings: A & B) Jejuno-jejunal intussusception caused by a pedunculated submucosal lipoma, measuring 50 mm.
Discussion
Intussusception is defined as the invagination of a proximal bowel segment into the lumen of an adjacent distal segment. The first case was reported in 1674 by Dr. Paul Barbette of Amsterdam [5]. Intussusception in adulthood is unusual with an incidence of approximately 2-3 cases per population of 1000000 per year. In contrast to pediatric intussusception, which is idiopathic in 90% of cases, adult intussusception presents an organic lesion (either benign or malignant) which serves as an apex for intussusception in 70% to 90% of cases [1, 6]. The most common classification system divides intussusceptions into four categories: enteric, ileocolic, ileocecal, and colonic [1]. While in the colon, the leading cause of intussusception is a primary carcinoma (65-70% of cases), intussusception in the small bowel is mainly caused by benign lesions such as leiomyomas, adenomas, lipomas, haemangiomas and fibromas. Less frequent causes in adults include adhesions, Meckel's diverticulum, and adenitis [7]. Lipomas are benign tumors of mesenchymal origin and they are the second most common benign tumors in the small intestine, accounting for 10% of all benign gastrointestinal tumors [8, 9]. There are three pathological types of intestinal lipomas: the intermuscular type, the subserosal type, and the submucosal type. The third one is the most common, accounting for more than 90% of intestinal lipomas [3].
According to literature, gastrointestinal lipomas are mainly located in the colon (64%) and small bowel (31%), less frequently in the esophagus (12%) and stomach (3%) [10]. Jejunal lipomas are rare (4-6% of all benign small bowel tumors) [10, 11]. In recent literature, out of 51 reported cases of gastrointestinal lipomas causing intussusception in adults, only 5 were reported arising from jejunum. [1, 12]. Most lipomas are solitary, however, in less than 10% of cases, multiple lipomas occur. [1, 13-15]. Gastrointestinal lipomas are rarely symptomatic while smaller than 2 cm. Larger intestinal lipomas can instead cause non-specific symptoms such as abdominal pain, diarrhea, and hematochezia. Acute manifestations (partial or complete bowel obstructions and/or bleeding), are infrequent occurrences. Bowel obstructions secondary to intestinal lipomas are caused by intussusception in the majority of documented case reports [10, 13].
The classic pediatric presentation of intussusception with the typical triad of abdominal pain, a sausage-shaped palpable mass and red jelly stools is rarely seen in adults. Adult intussusception usually has a non-specific presentation: it can have an acute, subacute, or chronic onset and it is rarely considered in the differential diagnosis for abdominal complaints [3, 4, 16]. Imaging is usually required to reach a diagnosis in case of intussusception in adulthood. Plain abdominal radiographs are of limited value, due to the low sensitivity and specificity. However, they are often performed as part of initial investigations for patients presenting with an acute abdomen. One of the radiographic features consistent with intussusception is signs of intestinal obstruction proximal to the lead point [7]. On ultrasound, the classical features include the ‘target’ or ‘doughnut’ sign on transverse view and “pseudo kidney” sign on longitudinal view, but image interpretation can be difficult in presence of air. Abdominal computed tomography is the most sensitive radiological method to confirm intussusception [13, 17]. On enhanced CT scan, an intussusception due to intestinal lipoma is seen as a well-circumscribed homogeneous lesion with attenuation value between -40 and -120 UH, typical for fat [6]. The sausage-shaped lesion, pathognomonic of intussusception, is visualized when the CT beam is parallel to its longitudinal axis, whereas the characteristic target-shaped lesion is visualized when the CT beam is perpendicular [7].
In contrast to colonic intussusception, where the lesion and the intussuscepted tract have to be mandatory resected en bloc, due to the high risk of malignancy, a selective, tailored approach can be applied for small bowel cases [7, 12]. The optimal surgical management remains controversial. Some investigators have stated that small bowel obstructions should be gently reduced only in patients in whom a definitive benign diagnosis has been made preoperatively. Intraoperative reduction of the intussusceptions prior to resection, may preserve a considerable length of bowel and thereby prevent the development of short-bowel syndrome [1]. If neoplasia, ischaemia or excessive oedema are the suspected cause of obstruction, segmentary resection (open or laparoscopic) without reduction must be performed and completed with primary anastomosis [5, 7, 16]. Partial obstructions can be managed conservatively with nihil per os, fluid resuscitation and nasogastric tube decompression. However, if there are no signs of improvement, operative intervention is recommended [18].
Conclusion
Intussusception in adults is an uncommon condition which, in most cases, has an organic cause, benign or malignant. Small bowel large lipoma (>2 cm) can cause intussusception presenting as obstruction. The diagnosis can be difficult because of atypical and non-specific symptoms. CT is the most useful tool for making a timely diagnosis, demonstrating intussusception and the fatty nature of the lesion acting as a lead-point. Surgical resection remains the treatment of choice.
Conflicts of Interest
None.
Author Contributions
P.A., M.C., A.F.A., M.M., P.B., A.S. drafted the manuscript, critically revised the manuscript, approved the final version to be published, and agree to be accountable for all aspects of the work. M.M. and P.B. interpreted the CT examination. All authors read and approved the final version of the manuscript.
Article Info
Article Type
Case ReportPublication history
Received: Fri 05, Feb 2021Accepted: Fri 19, Feb 2021
Published: Fri 05, Mar 2021
Copyright
© 2023 Paolo Aonzo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2021.03.03
Figures & Tables
References
1. Mouaqit O, Hasnai H, Chbani L, Benjelloun B, El Bouhaddouti H et al. (2012) Adult intussusceptions caused by a lipoma in the jejunum: report of a case and review of the literature. World J Emerg Surg 7: 28. [Crossref]
2.
Atila K, Terzi C,
Obuz F, Yilmaz T, Füzün M (2007) Symptomatic intestinal lipomas requiring
surgical interventions secondary to ileal intussusception and colonic
obstruction: report of two cases. Ulus Travma Acil Cerrahi Derg 13:
227-231. [Crossref]
3.
Jiang RD, Zhi XT,
Zhang B, Chen ZQ, Li T (2015) Submucosal lipoma: a rare cause of recurrent
intestinal obstruction and intestinal intussusception. J Gastrointest Surg
19: 1733-1735. [Crossref]
4.
Bentama K, Chemlal I, Benabbou M, El Abssi M, El Ouananni
M et al. (2012) Acute intussusception secondary to a lipoma of the small
intestine: about a case and review of the literature. Pan Afr Med J
12: 98. [Crossref]
5. Ahmed M, Habis S, Saeed R, Mahmoud A, Plurad D (2018) Submucosal lipomas causing intussusception and small bowel obstruction: A case report. Cureus 10: e3692. [Crossref]
6.
Vagholkar K, Chavan R, Mahadik A, Maurya I
(2015) Lipoma of the small intestine: a cause for intussusception in adults. Case
Rep Surg 2015: 856030. [Crossref]
7.
Patel S, Eagles
N, Thomas P (2014) Jejunal intussusception: a rare cause of an acute abdomen in
adults. BMJ Case Rep 2014: bcr2013202593. [Crossref]
8.
Krasniqi AS,
Hamza AR, Salihu LM, Spahija GS, Bicaj BX et al. (2011) Compound double
ileoileal and ileocecocolic intussusception caused by lipoma of the ileum in an
adult patient: A case report. J Med Case Rep 5: 452. [Crossref]
9.
Balamoun H, Doughan
S (2011) Ileal lipoma. A rare cause of ileocolic intussusception in adults:
Case report and literature review. World J Gastrointest Surg 3: 13-15. [Crossref]
10. Cuciureanu T, Huiban L, Chiriac S, Singeap AM, Danciu
M et al. (2019) Ulcerated intussuscepted jejunal lipoma-uncommon cause of
obscure gastrointestinal bleeding: a case report. World J Clin Cases 7:
3765-3771. [Crossref]
11. Lucas LC, Fass R, Krouse RS (2010) Laparoscopic
resection of a small bowel lipoma with incidental intussusception. JSLS
14: 615-618. [Crossref]
12. Seow En I, Foo FJ, Tang CL (2014) Jejunojejunal intussusception
secondary to submucosal lipoma resulting in a 5-year history of intermittent
abdominal pain. BMJ Case Rep 2014: bcr2014207297. [Crossref]
13. Minaya Bravo AM, Mansilla CV, Fraguas FN, Vincent
Granell FJ (2012) Ileocolic intussusception due to giant ileal lipoma: review
of literature and report of a case. Int J Surg Case Rep 3: 382-384. [Crossref]
14. Wan XY, Deng T, Luo HS (2010) Partial intestinal
obstruction secondary to multiple lipomas within jejunal duplication cyst: a
case report. World J Gastroenterol 16: 2190-2192. [Crossref]
15. Gao PJ, Chen L, Wang FS, Zhu JY (2014) Ileo-colonic
intussusception secondary to small-bowel lipomatosis: a case report. World J
Gastroenterol 20: 2117-2119. [Crossref]
16. Kabawe E, Kabawe S, Albakour R, Alobied M, Ghazal A (2019) Jejunal intussusception in an adult due to multiple lipomas: a rare case report from Syria. J Surg Case Rep 2019: rjz162. [Crossref]
17. Hanafiah M, Abdul Aziz M, Rusli SM (2019) Adult
entero-enteric intussusception secondary to lipoma. Clin Case Rep 7:
2267-2268. [Crossref]
18. Konik RD, Rhodes RA (2018) Complete small bowel
obstruction without intussusception due to a submucosal lipoma. J Surg Case
Rep 2018: rjy155. [Crossref]