A Rare Case of Rectal Gastrointestinal Stromal Tumor Associated with Parapharyngeal Metastasis
A Rare Case of Rectal Gastrointestinal Stromal Tumor Associated with Parapharyngeal Metastasis
A B S T R A C T
Background: Gastrointestinal stromal tumors are the most frequent mesenchymal tumors and represent 1-3% of all digestive neoplasms. Their incidence is 0.68 per 10,000 people. GISTs originate from the interstitial cells of Cajal, which are known as the gastrointestinal pacemaker, and carry mutations in the KIT gene in 95% of those affected. GISTs occur mainly in the middle-aged and rarely under the age of 40. The main age of presentation is 64 years old. The most common site of metastasis is the liver (65%), and exceptionally the bone (3%).
Discussion: Rectal GISTs represent 5 to 15% of all GISTs. They are usually asymptomatic and discovered incidentally. Surgical resection with curative intent is the standard treatment for localized GISTs. Complete excision of the tumor is the most significant factor related to the outcome and can be accomplished in 40-60% of cases. For borderline or unresectable lesions, neoadjuvant treatment with anti-tyrosine kinase (imatinib) should be considered. Imatinib is considered to be a relatively safe treatment and is generally well-tolerated by patients. Overall, the five-year survival rate is 90% for low-grade GIST, but the prognosis is worse for high-grade tumors (< 20%). Bone metastasis is a rare site of GIST metastases and usually presents itself during disease relapse. We present a rare case of a patient with an oligometastatic with pelvic bone lesion rectal GIST who developed parapharyngeal metastasis infiltrating C3 with airway compromise. Unfortunately, the patient passed away after massive tracheal bleeding.
Conclusion: Bone metastasis from GIST is uncommon. The development of dyspnea and hoarseness should prompt the diagnosis of potential life-threatening complications such as parapharyngeal metastasis.
Keywords
Rectal GIST, parapharyngeal metastasis, imatinib
Introduction
Stromal or mesenchymal neoplasms affecting the gastrointestinal (GI) tract typically present as subepithelial neoplasms. Among these tumors, gastrointestinal stromal tumors (GISTs) are the most frequent. Mesenchymal tumors account for 1% of all GI tumors. Sites of metastases include the liver (65%), the peritoneum, and in rare cases, the bone (3%) [1]. We report a rare case of rectal GIST associated with parapharyngeal metastasis.
Case Presentation
An 82-year-old man presented with a voluminous rectal GIST extending 2-14 cm from the anal verge with bone metastasis in the right iliac wing and lymph node metastases, which were confirmed by PET-CT (Figure 1). The therapeutical strategy was to start with neoadjuvant imatinib and in case of partial response to continue with radical rectal surgery and stereotactic radiotherapy on the bone lesion, with curative intent. During neoadjuvant treatment with imatinib (IM), the patient presented with Stevens-Johnson syndrome (SJS), and the treatment had to be discontinued. Restaging pelvic MRI (Figure 2) and PET-CT showed a very good partial response on the primary tumor and disappearance of the bone lesion. After a multidisciplinary discussion, considering the life-threatening side effect under imatinib, it was felt that surgery was the only therapeutic option, and abdominoperineal resection was performed in August 2019. The operation was complicated by intraoperative bleeding requiring multiple blood transfusions and postoperative wound dehiscence requiring VAC therapy and subsequent advancement flap (Figure 3). The tumor was perforated, and the resection margins were considered as R1.
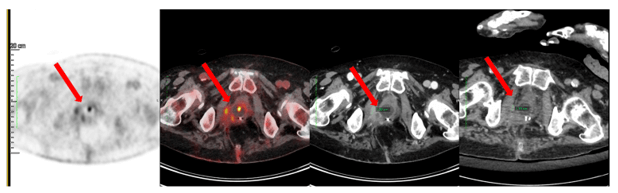
Figure 1: PET-scan image of the rectal GIST.

Figure 2: Restaging MRI image of the rectal GIST.

Figure 3: Reconstruction after abdominoperineal resection, postoperative wound dehiscence requiring VAC therapy and subsequent advancement flap.
In November 2019, the patient presented with progressive dysphagia and dysphonia. The cervical CT and MRI scan showed a new parapharyngeal lesion infiltrating C3 (Figure 4). The biopsies confirmed a metastatic GIST. A tracheostomy was required to secure the airway. While awaiting treatment with a new anti-tyrosine kinase therapy and radiotherapy, the patient deteriorated quickly. Unfortunately, he had massive upper airway bleeding and passed away.

Figure 4: MRI image of the parapharyngeal mass originating from a paravertebral muscle and infiltrating C3 compressing the upper airway.
Discussion
GISTs are the most frequently occurring mesenchymal tumors of the digestive tract. They can appear from the oesophagus to the anus and more rarely from the peritoneal cavity or mesentery, with the most common site being the stomach (40-60%) [2, 3]. Rectal GISTs are uncommon and appear in 5 to 15% of cases. They are usually asymptomatic and are discovered incidentally during an endoscopic study or on cross-sectional imaging done for another reason. Mostly, they are associated with non-specific symptoms (early satiety, bloating and bleeding). In the case of large rectal GISTs, they can be associated with abdominal pain or obstruction [4]. The majority of rectal GISTs presents as a small and hard nodule. Large rectal GISTs can ulcerate and imitate a rectal adenocarcinoma with rectal bleeding, abdominal discomfort and constipation [5]. Only tumors smaller than two cm and with a mitotic rate less than 5 per 50 high power fields (HPFs) seem to carry a low risk of distant metastases. On the other hand, even small, but mitotically active (> 5 per 50 HPFs) GISTs in the rectum have a metastatic rate greater than 50% [3].
For the treatment of rectal GISTs, surgical resection with histologically negative margins remains the mainstay [6]. Resection of rectal GISTs can be surgically difficult and is associated with considerable morbidity. Along with the confined pelvic space, complete surgical resection can be difficult to achieve, especially when rectal GISTs are large tumors and densely adherent to the pelvic floor musculature and surrounding organs [7]. A transanal resection is the first choice for small GISTs located within 5 cm of the anal verge. The trans-sacral approach can be an option for lesions located in the middle portion of the rectum [8]. A transvaginal approach is an option for local excision of rectal GISTs in the anterior wall of the rectum or rectovaginal septum in female patients. These two approaches allow safe resection of the tumor with low morbidity and spare the patient from abdominoperineal amputation [9]. These different options are possible because a formal mesorectal excision is not necessary, as lymphatic metastases are rare.
Depending on the size of the GIST and its exact location, when local resection is not possible, a formal low anterior resection with a coloanal anastomosis is required. For bigger lesions in the low rectum, an abdominoperineal resection is often necessary to accomplish a complete oncological resection. A total or posterior exenteration is sometimes mandatory when the tumor is fixed to the surrounding pelvic structures. For our patient, we performed an abdominoperineal resection due to the large size and localization in the low rectum without the possibility of sphincter preservation. In large (> 5 cm) and high-risk (> 5 per 50 HPFs) rectal GISTs, IM, a tyrosine kinase inhibitor (TKI) that specifically inhibits most KIT- and PDGFRA-activated proteins, has been used as neoadjuvant therapy. It helps to downstage the tumors, and it improves the chance of radical surgery and disease-free survival (DFS) [10]. In the series of Liu, tumors with mitotic rates < 5 per 50 HPFs and negative resection margins were favourable factors for DFS [11]. Perioperative imatinib therapy for the patients with tumor size greater than 5 cm could increase the rate of negative margin resections and for intermediate or high-risk tumors is associated with a prolonged DFS [12].
The incidence of bone metastasis is 3%. The most common sites are the spine and pelvis [13]. Usually, liver metastasis is already present when bone metastasis appears [14]. Bone metastasis is diagnosed rarely at disease presentation and more frequently at disease relapse [15]. Tumor spread may occur continuously, or by lymphatic spread, or by intravascular dissemination. The exact mechanism remains unknown [16]. IM is the treatment of choice for metastatic or unresectable GISTs. Treatment with IM is generally well-tolerated, even if patients may have mild to moderate adverse effects, such as oedema (74%), nausea (52.4%) and diarrhoea (44.9%). The most serious adverse events were GI or intraabdominal haemorrhage in patients with large, bulky tumors, which occurred in approximately 5% of patients [17]. Similarly, a phase II study in Japan also found that IM was generally safe for advanced GISTs [18]. Unfortunately, our patient experienced SJS after his IM treatment, and it had to be discontinued. SJS is a severe, life-threatening adverse cutaneous reaction related to medications, with a mortality rate below 5% [19].
It is rare, occurring in 0.01-0.1% of the time. These adverse cutaneous reactions typically occur 9 days and 2 months after starting IM at daily doses of 400-600 mg [20]. Our patient’s treatment required the immediate discontinuation of IM with hospitalization and the addition of systemic steroid therapy [21]. A minimum of 6-12 months of neoadjuvant treatment with IM is recommended to be effective [22]. IM has shown efficacy in bone metastases of GISTs, with a 19-month response [23]. Kanda et al. reported a five-year overall survival (OS) of 60.9% and median survival of 70 months, with a median follow-up of 68 months after IM therapy for advanced GISTs [24]. Perioperative IM was associated with improved local DFS, overall DFS and OS. In a series of 36 patients with rectal GISTs treated with surgery, five (13.9%) developed a local recurrence within a median of 12 months. The patients with local recurrence had not undergone curative resection and had not received perioperative IM therapy [12].
In our case, the surgery had an R1 resection margin, and the patient could not finish the perioperative IM treatment. After an initially good postoperative evolution, the patient developed progressive dysphagia and dysphonia three months later. The investigation revealed a new parapharyngeal lesion infiltrating C3, which was confirmed to be a GIST metastasis. Skeletal muscle metastasis of GISTs is really rare. Only four cases have been reported in the literature, and only one was a paravertebral muscle metastasis [25]. None of these were a parapharyngeal mass originating from a paravertebral muscle and infiltrating C3. After a multidisciplinary discussion, we opted for systemic treatment. Indeed, surgery was not an option because of the location and size of the metastasis. Due to the previous severe reaction to IM, we started a second-line treatment with sunitinib. In the literature, sunitinib is a second-line drug approved for IM-resistant GISTs and is associated with a clinical benefit rate of about 50% and a DFS of 7-10 months [26].
Newer second-generation TKIs, such as nilotinib and dasatinib, are also considered safe in patients intolerant to IM because of a lack of cross-reactivity [21, 27]. Even if GISTs are not radiosensitive tumors, radiotherapy can be used for palliative purposes, as we intended in our patient [28]. Bisphosphonates can also be used as an effective treatment for bone metastases of GISTs [15]. The parapharyngeal metastasis, due to its specific location, was responsible for an extrinsic compression of the oropharynx and hypopharynx. Depending on the patient’s general condition and the site and type of metastasis, various treatments are available in order to secure the upper airway (e.g., airway stents, laser, radiotherapy and tracheostomy) [29].
In our case, we decided on a surgical tracheostomy. Even with this measure, the tumor eroded an important neck vessel, and the patient presented with massive upper airway bleeding that led to his death. Our case was challenging because it did not follow a classic evolution. The severe cutaneous reaction interrupted perioperative treatment with IM, which is indicated in metastatic GISTs. The size of the rectal GIST forced us to technically obtain an R1 margin resection. Postoperatively, the patient presented with a rare parapharyngeal metastasis for which the treatment was again challenging due to the situation (the size and location of the metastasis and the severe reaction to IM).
Conclusion
To conclude, rectal GISTs are rare mesenchymal tumors of the GI tract. Rectal GISTs with bone metastases are even rarer. Surgical resection with an R0 resection margin and neoadjuvant IM is the treatment of choice for large and high-risk tumors. IM remains the treatment of choice for bone metastases, although it can result in some rare severe cutaneous adverse effects. Multi-metastatic GIST remains a challenging case where for which the therapeutic approach and the follow-up should be discussed during a multidisciplinary meeting.
Article Info
Article Type
Case ReportPublication history
Received: Wed 15, Jul 2020Accepted: Tue 28, Jul 2020
Published: Wed 12, Aug 2020
Copyright
© 2023 Sleiman Marwan Julien. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.08.07
Figures & Tables
References
- Satoshi Hamada, Atsushi Itami, Go Watanabe, Shinya Nakayama, Eiji Tanaka et al. (2010) Intracranial metastasis from an esophageal gastrointestinal stromal tumor. Intern Med 49: 781-785. [Crossref]
- M Miettinen, Jerzy Lasota (2001) Gastrointestinal stromal tumors--definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch 438: 1-12. [Crossref]
- Markku Miettinen, Jerzy Lasota (2006) Gastrointestinal stromal tumors: pathology and prognosis at different sites. Semin Diagn Pathol 23: 70-83. [Crossref]
- Markku Miettinen, Leslie H Sobin, Jerzy Lasota (2005) Gastrointestinal stromal tumors of the stomach: a clinicopathologic, immunohistochemical, and molecular genetic study of 1765 cases with long-term follow-up. Am J Surg Pathol 29: 52-68. [Crossref]
- A Manouras, A Pappas, V Katergiannakis, K Filis, J Chrysikos et al. (2009) Gastrointestinal stromal tumors of the rectum: report of five cases. Acta Gastroenterol Belg 72: 257-261. [Crossref]
- Roberto Logroño, Dennie V Jones, Sohaib Faruqi, Manoop S Bhutani (2004) Recent advances in cell biology, diagnosis and therapy of gastrointestinal stromal tumor (GIST). Cancer Biol Ther 3: 251-258. [Crossref]
- P Gervaz, O Huber, P Morel (2009) Surgical management of gastrointestinal stromal tumours. Br J Surg 96: 567-578. [Crossref]
- P Gervaz, O Huber, P Bucher, P Sappino, P Morel (2008) Trans‐sacral (Kraske) approach for gastrointestinal stromal tumour of the lower rectum: old procedure for a new disease. Colorectal Dis 10: 951-952. [Crossref]
- Minia Hellan, Vijay K Maker (2006) Trans‐vaginal excision of a large rectal stromal tumor: an alternative. Am J Surg 191: 121-123. [Crossref]
- Heikki Joensuu, Mikael Eriksson, Kirsten Sundby Hall, Jörg T Hartmann, Daniel Pink et al. (2012) One vs three years of adjuvant imatinib for operable gastrointestinal stromal tumor: a randomized trial. JAMA 307: 1265-1272. [Crossref]
- Heli Liu, Zhongshu Yan, Guoqing Liao, Hongling Yin (2014) Treatment strategy of rectal gastrointestinal stromal tumor (GIST). J Surg Oncol 109: 708-713. [Crossref]
- Jens Jakob, Chiara Mussi, Ulrich Ronellenfitsch, Eva Wardelmann, Tiziana Negri et al. (2013) Gastrointestinal stromal tumor of the rectum: results of surgical and multimodality therapy in the era of imatinib. Ann Surg Oncol 20: 586-592. [Crossref]
- Anupma Jati, Servet Tatlı, Jeffrey A Morgan, Jonathan N Glickman, George D Demetri et al. (2012) Imaging features of bone metastases in patients with gastrointestinal stromal tumors. Diagn Interv Radiol 18: 391-396. [Crossref]
- Kayo Suzuki, Taketoshi Yasuda, Kaoru Nagao, Takeshi Hori, Kenta Watanabe et al. (2015) Bone metastasis of a gastrointestinal stromal tumor: a report of two cases. Oncol Lett 9: 1814-1818. [Crossref]
- Valerio Di Scioscio, Laura Greco, Maria Caterina Pallotti, Maria Abbondanza Pantaleo, Alessandra Maleddu et al. (2011) Three cases of bone metastases in patient with gastrointestinal stromal tumors. Rare Tumors 3: e17. [Crossref]
- Judith R Kroep, Judith V M G Bovée, Aart J van der Molen, Pancras C W Hogendoorn, Hans Gelderblom (2009) Extra-abdominal subcutaneous metastasis of a gastrointestinal stromal tumor: report of a case and a review of the literature. J Cutan Pathol 36: 565-569. [Crossref]
- George D Demetri, Margaret von Mehren, Charles D Blanke, Annick D Van den Abbeele, Burton Eisenberg et al. (2002) Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med 347: 472-480. [Crossref]
- Toshirou Nishida, Kuniaki Shirao, Akira Sawaki, Masato Koseki, Takeshi Okamura et al. (2008) Efficacy and safety profile of imatinib mesylate (ST1571) in Japanese patients with advanced gastrointestinal stromal tumors: a phase II study (STI571B1202). Int J Clin Oncol 13: 244-251. [Crossref]
- J C Roujeau, R S Stern (1994) Severe adverse cutaneous reactions to drugs. N Engl J Med 331: 1272-1285. [Crossref]
- Huei Jen Hsieh, Agnes L F Chan, Shun Jen Lin (2009) Stevens-Johnson syndrome induced by combination of imatinib and allopurinol. Chemotherapy 55: 197-199. [Crossref]
- Alfonso Quintás Cardama, Jorge E Cortés, Hagop Kantarjian (2008) Practical management of toxicities associated with tyrosine kinase inhibitors in chronic myeloid leukemia. Clin Lymphoma Myeloma 8: S82-S88. [Crossref]
- Ronald Tielen, Cornelis Verhoef, Frits van Coevorden, Anna K. Reyners, Winette T.A. van der Graaf et al. (2012) Surgical management of rectal gastrointestinal stromal tumors. J Surg Oncol 107: 320-323.
- Michael Stamatakos, Emmanouel Douzinas, Charikleia Stefanaki, Panagiotis Safioleas, Electra Polyzou et al. (2009) Gastrointestinal stromal tumor. World J Surg Oncol 7: 61. [Crossref]
- Tatsuo Kanda, Takashi Ishikawa, Seiichi Hirota, Kazuhito Yajima, Shin ichi Kosugi et al. (2012) Prospective observational study of imatinib therapy in Japanese patients with advanced gastrointestinal stromal tumors: long-term follow-up and second malignancy. Jpn J Clin Oncol 42: 578-585. [Crossref]
- Kayo Suzuki, Taketoshi Yasuda, Kaoru Nagao, Takeshi Hori, Kenta Watanabe et al. (2014) Metastasis of gastrointestinal stromal tumor to skeletal muscle: a case report. J Med Case Rep 8: 256. [Crossref]
- George D Demetri, Allan T van Oosterom, Christopher R Garrett, Martin E Blackstein, Manisha H Shah et al. (2006) Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet 368: 1329-1338. [Crossref]
- Guoqing Wei, Shamudheen Rafiyath, Delong Liu (2010) First-line treatment for chronic myeloid leukemia: dasatinib, nilotinib, or imatinib. J Hematol Oncol 3: 47. [Crossref]
- C D Blanke, B L Eisenberg, M C Heinrich (2001) Gastrointestinal stromal tumors. Curr Treat Options Oncol 2: 485-491. [Crossref]
- Linda Shavit, Bella Maly, Eli Rosenbaum, Tal Grenader (2007) Endotracheal metastases in renal cell carcinoma: a life-threatening but treatable complication. Eur J Intern Med 18: 161-163. [Crossref]