A Huge Endocarditis Pseudoaneurysm in Bicuspid Aortic Valve
A B S T R A C T
Infective endocarditis is a disease associated with high mortality and severe complications. We report a case of a young shepherd affected by valvular endocarditis on a bicuspid aortic valve, complicated by a pseudoaneurysm with periaortic abscess. Thanks to the use of multimodality diagnostic imaging (particular echocardiogram, Magnetic Risonance Imaging, Computed tomography-scan and coronary angiography), it was possible to make a correct diagnosis, in order to plan a tailored surgical strategy and to reduce the perioperative risks. The operation consisted of myocardial revascularization, closure of the annular pseudoaneurysm and aortic valve replacement with mechanical prosthesis. The patient maintained normal inflammation indices and was discharged at home in the absence of relevant clinical events. Infective endocarditis is a deadly disease. Multimodality imaging is crucial to clarify anatomical distorsions that can occur in complicated cases.
Keywords
Bicuspid aortic valve, echocardiography, endocarditis, valve disease
Case Report
We reported the clinical case of a 31 years old shepherd, with a past history of asymptomatic aortic bicuspid valve. On February 2017, he referred to the Emergency Department because of persistent fever for a month associated with worsening dyspnoea and ankle swelling; he therefore underwent cardiologic evaluation and transthoracic echocardiographic examination, which revealed a vegetation on the bicuspid aortic valve with severe aortic regurgitation and probable periaortic abscess. In order to exclude acute aortic syndrome, a computed tomography angiography was performed: it ruled out any intimal flaps or dissections of both thoracic and abdominal aorta; however, the scan highlighted a voluminous paravalvular pseudoaneurysm. No acute cerebral parenchymal lesions were found on CT brain scanning. The patient was therefore admitted to cardiac surgery unit with the diagnosis of infective endocarditis; blood culture performed on admission revealed the presence of Staphylococcus Hominis then antibiotic therapy with vancomycin and gentamicin was started.
The transesophageal echocardiographic examination showed bicuspid aortic valve characterized by the fusion of the right and non-coronaric cusps (type 2 bicuspid valve) with severe regurgitation, due to an highly mobile vegetation attached to ventricular surface of the anterior cusp; it also revealed a voluminous abscess near to the right coronary sinus [1]. For this reason, irrespective of age, the patient underwent coronary angiography, which showed dominant right coronary artery, characterized by a proximal ab extrinsic compression of its lumen (70% stenosis) (Figure 1); no stenosis were found in left coronary artery, anterior descending artery and circumflex artery. In order to understand the anatomic and spatial features of the endocarditis mass, a cine angiothoracic magnetic resonance was performed; it showed a huge paravalvular pseudoaneurysm (DT 50x49 mm) between right and non coronaric cusps, communicating with aortic root (10 mm) and causing severe aortic regurgitation; it also confirmed the normal caliber of the thoracic aorta and the normal origin of the sovraortic vessels. The patient was then scheduled for cardiac surgery intervention. After median sternotomy, intraoperative exploration showed a voluminous mass emerging from the right ventricle and determining severe compression of the right atrium in its auricular portion (Figure 2). First, the right coronary artery was bypassed with a safenous vein graft during beating heart, to avoid ischemic injury for right portion of the heart during cardioplegic delivery. After cardiopulmonary bypass institution and cold blood cardioplegia solution delivered, the aortotomy showed a severely degenerated bicuspid aortic valve because of an endocarditic process.

Figure 1: Coronary Angiography showed proximal ab extrinsic compression of right coronary artery.
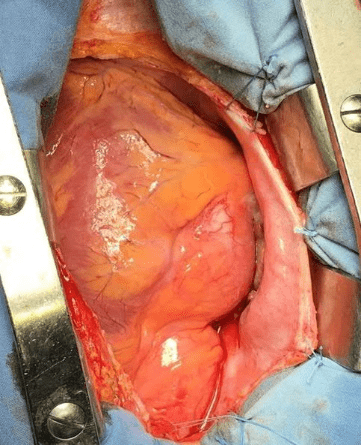
Figure 2: Intraoperative view showing a voluminous mass emerging from the right ventricle and determining severe compression of the right atrium in its auricular portion.
Moreover, just above the valvular annulus, between the right coronary and non-coronary sinus, a fistula feeds a voluminous abscess cavity with a pseudo-aneurysm aspect. Aortic valve replacement was carried out with a mechanical prosthesis (Sorin Bicarbon 21 mm) and the abscess cavity was closed with pericardial patch. Weaning from cardiopulmonary bypass was easy and the patient was transferred to intensive care under satisfactory haemodynamic conditions. After about 8 hours, the patient was extubated and after 24 hours he was transferred to the hospital ward. The next course has been regular. The patient was then transferred to Cardiovascular Rehabilitation Unit for the continuation of treatment (antibiotic therapy and rehabilitation). During the hospitalization, a daptomycin-induced neutropenia occurred, so therapy with corticosteroids medications had started with benefit (absolute neutrophil count raise from 520 cells/µL to 5100 cells/µL). In relation to the negativity of the inflammation indices, the worsening of the renal function indices and the absence of fever during the entire hospital stay, as well as the appropriate duration of antibiotic therapy (> 6 weeks), daptomycin administration was then suspended; the control blood culture performed in pre-discharge was negative for bacterial and mycotic growth. To date the patient had no further complications.
Discussion
Infective endocarditis is a disease associated with high mortality and severe complications. Patients with bicuspid aortic valve are known to be at intermediate risk for infective endocarditis and dental and cutaneous hygiene should be mandatory. The patient described was a shepherd and was unaware of his aortic valve pathology until infective endocarditis developed. The use of different imaging techniques during pre-operative evaluation allows cardiac surgeon to understand spatial relationships between endocarditis mass and anatomical structures, reduces pre-operative risks and post-operative complications and optimizes surgical timing, as in our case report. The need for prolonged antibiotic therapy increases the risk for antibiotic-induced neutropenia [2-5]. Monitoring of neutrophil count should be mandatory, especially in patients treated with beta-lactam antibiotics and daptomicin.
Conflicts of interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Tue 24, Sep 2019Accepted: Tue 08, Oct 2019
Published: Fri 18, Oct 2019
Copyright
© 2023 Giuseppe Vitale. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JICOA.2019.04.04
Figures & Tables
References
- Schaefer BM, Lewin MB, Stout KK, Gill E, Prueitt A et al. (2008) The bicuspid aortic valve: an integrated phenotypic classification of leaflet morphology and aortic root shape. Heart 94: 1634-1638. [Crossref]
- Duval X, Leport C (2008) Prophylaxis of infective endocarditis: current tendencies, continuing controversies. Lancet Infect Dis 8: 225-232. [Crossref]
- Feuchtner GM, Stolzmann P, Dichtl W, Schertler T, Bonatti J et al. (2009) Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J Am Coll Cardiol 53: 436-444. [Crossref]
- Koo HJ, Yang DH, Kang JW, Lee JY, Kim DH et al. (2018) Demonstration of infective endocarditis by cardiac CT and transoesophageal echocardiography: comparison with intra-operative findings. Eur Heart J Cardiovasc Imaging 19: 199-207. [Crossref]
- Olaison L, Belin L, Hogevik H, Alestig K (1999) Incidence of B-Lactam-induced delayed hypersensitivity and neutropenia during treatment of infective endocarditis. Arch Intern Med 159: 607-615. [Crossref]