A Case of Leukemia Cutis in an Inguinal Herniorraphy Scar
A B S T R A C T
Leukemia cutis refers to the infiltration of the skin with leukemia cells. It is a rare extramedullary manifestation of leukemia, but it is a specific sign of disease progression and bad prognosis. Cases of leukemia cutis in sites of skin trauma or surgical scars have been described, but there are very few cases reported in literature. We report a case of a 65-year-old male previously diagnosed with chronic myelomonocytic leukemia that was showing clinical signs of progression to acute myeloid leukemia. He underwent right inguinal herniorrhaphy three months before and was showing poor wound healing. Surgical site infection was suspected, since blood tests showed prolonged neutropenia, so surgical wound debridement was performed. Pathological findings of removed tissue indicated infiltration by leukemic cells, which led to the diagnosis of leukemia cutis, not suspected until that moment. Therefore, we conclude that an exhaustive skin examination (especially in the presence of skin trauma or surgical scars), should be performed in patients with confirmed or suspected diagnosis of leukemia. Moreover, the possible diagnosis of leukemia cutis should be considered in leukemia patients who present cutaneous infectious complications or suboptimal healing following accidental skin trauma or surgery. In these cases, complementary anatomopathological studies should be performed.
Keywords
Leukemia cutis, chronic myelomonocytic leukemia (CMML), acute myeloid leukemia (AML), inguinal herniorrhaphy, surgical scar, scar debridement, scar infection
Introduction
Leukemia cutis is an extramedullary manifestation that can be found in some types of leukemia, especially in acute myeloid leukemia. It is defined as the infiltration of the skin by neoplastic cells or its precursors [1]. The diagnosis is confirmed by anatomopathological study of the skin and is strongly associated with acute progression and low life expectancy [2]. Some theories suggest the existence of an affinity of neoplastic cells for skin injuries, but very few cases of leukemia cutis at the site of surgical scars have been reported.
The purpose of this case report is to highlight an uncommon case of an inguinal herniorrhaphy scar that was not healing properly, and despite suspicion of infectious complications, finally pathological findings revealed the presence of leukemia cells in removed tissue from the scar, which confirmed the diagnosis of leukemia cutis.
Case Presentation
A 65-year-old male was diagnosed in 2015 with chronic myelomonocytic leukemia (CMML) type 1, with intermediate-1 risk. Allogenic hematopoietic stem cells transplant was contraindicated because of recent history of cancer (melanoma in 2012), so wait and see attitude was adopted. But one year later, the patient showed signs of disease progression, so treatment with Hydrea was initiated.
Two years later, in April 2018, due to detection of persistent pancytopenia, the patient was admitted in our hospital with diagnostic orientation of progression of his CMML to acute myeloid leukemia (AML). Bone marrow biopsy was performed and confirmed the diagnosis of AML. Pathological findings showed infiltration of bone marrow by myeloid leukoblasts, with important trilinear dysplasia. Chemotherapy was started, using IDEA therapy (Idarubicin, Cytarabine and Etoposide), without short-term side effects. Moreover, it is important to note that previously, in February 2018, the patient underwent a surgery. Actually, right inguinal herniorrhaphy was performed, but surgical wound showed poor post-operative scarring within the next two months. That is the reason why CT scan was performed during hospital stay and revealed the presence of a fluid collection at surgical site (Figure 1).

Figure 1: Computed tomography scan (pelvic cut) shows the presence of a fluid collection at surgical site.
Both radiological and blood test (prolonged neutropenia) findings led to the suspicion of surgical site infection, so surgical wound examination and debridement was performed: a great amount of necrotic and slough tissue was removed during surgery (Figure 2). Microbiological analysis report informed about presence of S. epidermidis and E. faecium, which were treated with Vancomycin during hospital stay and Ciprofloxacin once the patient was discharged, after significant improvement. Anatomopathological report described extensive dermo epidermal necrosis, with haemorrhagic areas in the dermis, and presence of interstitial and intravascular infiltrate, made of cells with large nuclei, rough chromatin, and little cytoplasm, with blast morphology and CD6 positivity. These findings, although not expected, were compatible with the diagnosis of leukemia cutis in an inguinal herniorrhaphy scar.
Unfortunately, the patient showed progression of his leukemia despite several lines of chemotherapy, so poor short-term prognosis is expected.
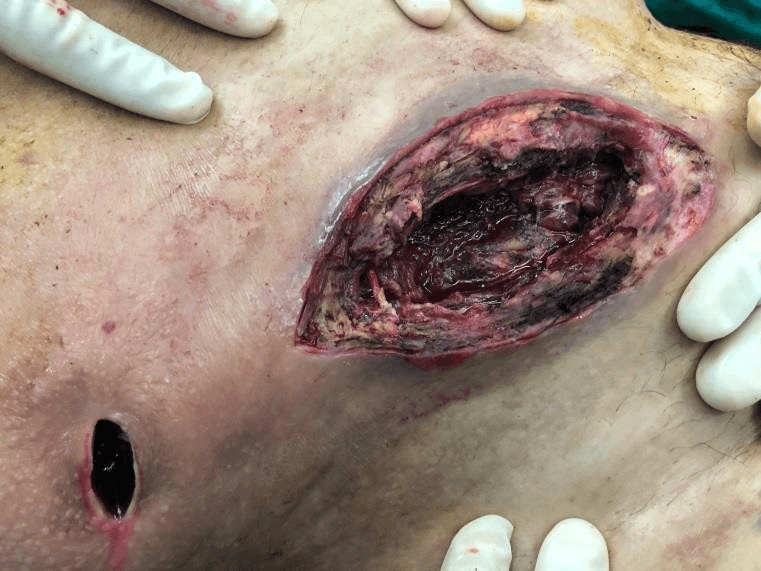
Figure 2: Appearance of the right inguinal herniorrhaphy wound during debridement surgery.
Discussion
Leukemia cutis is the infiltration of neoplastic leukocytes or their precursors into epidermis, dermis, or subcutaneous tissue [1]. The diagnosis is confirmed by skin biopsy and immunohistochemistry [2]. In most cases, there are perivascular or diffuse infiltrate, which affect dermis and subcutaneous tissue, but don’t affect the upper part of papillary dermis [3]. Nevertheless, histological findings can be very variable and don’t always correlate with clinical findings [2, 4]. Leukemia cutis is considered as a specific cutaneous leukemia manifestation, since neoplastic cells can be found in skin lesions. It differs from unspecific cutaneous leukemia manifestations, which are more common but instead no neoplastic cells could be found in a biopsy. Some examples of unspecific cutaneous leukemia manifestations would be inflammatory lesions, paraneoplastic syndromes and citopenias’ manifestations (haemorrhages, infections, etc.) [1, 4-6].
Acute myeloid leukemia is the type of leukemia where this clinical manifestation is more often found, with an incidence between 2.9 and 3.7%. This incidence can be increased to 10-50% in case of myelomonocytic leukemia (AML-M4) and monocytic leukemia (AML-M5); which are also associated with gingival and meningeal infiltration [1, 3, 6-8]. Some studies suggest that monocytes have biological characteristics that provide them with greater adhesive, phagocytic and deformable capacity, compared to other white blood cells. This allows them to adhere and pass through vascular endothelial cells more easily, and therefore invade extravascular locations [6, 7]. Leukemia cutis can only be found in between 1.3 and 3% of patients with lymphocytic leukemia and has a very low incidence in chronic myelomonocytic leukemia (CMML) [7]. In CMML, it is a sign of leukemia’s progression or transformation to its acute phase, and therefore it is a clear sign of bad prognosis [4].
Cases of leukemia cutis in sites of skin trauma have been described, such as surgical wounds, recent injuries, intravenous catheters insertion sites, intramuscular injection sites, burns, herpetic whitlows and other types of scar tissue [1, 6, 7]. But very few cases have been reported in scientific literature (such as our case report), which justifies why the real incidence remains unknown.
Different theories try to explain why neoplastic cells might have affinity for traumatic regions. It is thought that vascular endothelial damage and increased blood flow in the area of damaged tissue may increase the adherent capacity of inflammatory blood cells to blood vessel cells (it may affect either healthy white blood cells, and neoplastic cells) [5, 7, 8].
Leukemia cutis is associated with extramedullary involvement in other locations, and also with specific cytogenetic mutations. It is a sign of poor prognosis, with a life expectancy between 1.3 and 3.6 months after its diagnosis [2-6, 8]. It is also associated with a higher rate of recurrence, which suggests that skin lesions can be used as a reservoir for neoplastic cells, as a way to protect themselves from various treatments [1, 5]. When there is actually a recurrence, leukemia cutis can be the very first clinical manifestation before any other systemic symptoms or signs. That is the reason why an exhaustive skin examination is always necessary in this type of patients, paying special attention to scars, especially if they are not healing properly or if a scar infection is suspected [6].
Conclusion
Leukemia cutis is not a very common extramedullary manifestation of leukemia, but it can be its first manifestation, or a sign of recurrence, and it is a clear sign of short-term bad prognosis. Therefore, an exhaustive skin examination should be performed in patients who are diagnosed of leukemia, either confirmed or suspected, even if they are in complete remission. It is a diagnosis that should be suspected in patients diagnosed with leukemia who have skin injuries or surgical scars that are not properly healing or suspected to be infected. In these cases, anatomopathological study should be performed.
Conflicts of Interest
None.
Funding
None.
Ethical Approval
Not Applicable.
Author Contributions
All authors have substantially contributed to conducting the underlying research and drafting this manuscript, and the final version has been read and approved for submission in Surgical Case Reports (SCR) by all of them.
Article Info
Article Type
Case ReportPublication history
Received: Wed 20, May 2020Accepted: Sat 06, Jun 2020
Published: Fri 19, Jun 2020
Copyright
© 2023 Ivette Tort Estruch. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.06.12
Figures & Tables
References
- Angoori G Rao, Indira Dantury (2012) Leukemia cutis. Indian J Dermatol 57: 504. [Crossref]
- Li Li, Yanan Wang, Christine Guo Lian, Nina Hu, Hongzhong Jin et al. (2018) Clinical and pathological features of myeloid leukemia cutis. An Bras Dermatol 93: 216-221. [Crossref]
- R M Guinovart, J M Carrascosa, C Ferrándiz (2010) Leucemia cutis desarrollada en la zona de inoculación de una dosis de recuerdo de la vacuna del tétanos. Actas Dermo-Sifilográficas 101: 727-729.
- Francisco Javier Saldívar Alarcóna, José Luis del Burgo Fernández (2012) Un paciente con. leucemia cutis. Rev Clín Med Fam 5: 206-208.
- Gunnar Wagner, Klaus Fenchel, Walter Back, Alina Schulz, Michael Max Sachse (2012) Leukemia cutis – epidemiology, clinical presentation, and diferential diagnoses. J Dtsch Dermatol Ges 10: 27-36. [Crossref]
- H Koizumi, M Kumakiri, M Ishizuka, A Ohkawara, S Okabe (1991) Leukemia cutis in acute myelomonocytic leukemia: infiltration to minor traumas and scars. J Dermatol 18: 281-285. [Crossref]
- Jae In Lee, Hyung Jeong Park, Sin Taik Oh, Jun Young Lee, Baik Kee Cho (2009) A case of Leukemia Cutis at the Site of a Prior Catheter Insertion. Ann Dermatol 21: 193-196. [Crossref]
- Hei Sung Kim, Min Jee Choi, Hyung-Ok Kim, Young Min Park (2010) Leukemia cutis limited to the needle puncture sites. J Dermatol 37: 393-395. [Crossref]