A Case of Colonic Ischaemia Masquerading as a Colonic Mass
A Case of Colonic Ischaemia Masquerading as a Colonic Mass
A B S T R A C T
Intestinal ischaemia is an uncommon vascular syndrome resulting from an acute or chronic drop in blood supply to the bowel, with varied clinical presentations. Intestinal ischaemia can present similarly to other conditions, leaving the clinician with a diagnostic dilemma. In this case report, we present a 69-year-old male who presented with abdominal pain, distention, anorexia and per rectal bleeding. Endoscopy showed a left-sided mass-like, ulcerated lesion, endoscopically thought to be colonic carcinoma. Histology later revealed this mass to be intestinal ischaemia, with no features of invasive carcinoma. This was confirmed at an interval endoscopy, which showed a largely healed mucosa and nil evidence of a mass. Raising awareness of this disease and its ability to mimic other presentations, both clinically and endoscopically, is key to establishing an early diagnosis and intervention.
Keywords
Intestinal ischaemia, colonic carcinoma, abdominal pain, endoscopy, ischaemic colitis, colonic ischaemia
Introduction
Intestinal ischaemia is an uncommon vascular syndrome that is associated with high mortality. Ischaemic colitis can mimic other presentations such as inflammatory bowel disease or colorectal carcinoma. Its endoscopic appearance can be indistinguishable from these diagnoses and requires a histological diagnosis to be made in the right clinical context in order to exclude other causes. Our case brings forth the challenges in diagnosing this clinical entity and underscores the importance of including it among differential diagnosis.
Case Report
A 69-year-old Caucasian male presented to the emergency department of our hospital with cramping abdominal pain, distention, anorexia and per rectal bleeding for the preceding four days. The abdominal pain was mostly postprandial. His medical background included a history of ischemic heart disease, chronic obstructive lung disease and hypothyroidism. He had a 20 pack-year history of smoking and consumed 30 units of alcohol per week. Laboratory investigations showed leukocytosis, mild anaemia and raised inflammatory markers, noted in (Table 1).
Table 1: Laboratory values.
|
Laboratory values |
Values (normal range) |
|
White cell count |
16.9 x 109 cells/L (4.0-11.0) |
|
Haemoglobin |
11.6 g/dL (12.5-17.5) |
|
Mean corpuscular volume |
86.3 fL (79.0-96.0) |
|
Platelets |
280 x 109 cells/L (140-400) |
|
C-reactive protein |
55 mg/L (<5) |
|
Liver function tests |
Normal |
|
Urea, creatinine and electrolytes |
Normal |
|
Stool Culture |
Negative |
|
Clostridium difficile |
Negative |
|
Faecal calprotectin |
>6000 µg/g (<50) |
|
Lactate |
3.3 mmol/L (<2.2) |
CT abdomen and pelvis with contrast showed non-specific colitis of the descending colon. Coronal and axial cuts are shown in (Figures 3 & 4). Following this, he underwent a sigmoidoscopy that showed a large mass-like ulcerated lesion in the descending colon. This involved about 15 cm of the colon and occupied about 30% of the lumen, as shown in (Figure 1). Histology was suggestive of ischaemic colitis (Figures 5-8). The multidisciplinary meeting recommended an interval colonoscopy which showed resolution of the colonic mass lesion (Figure 2). He was fluid resuscitated and started on empiric broad-spectrum antibiotics.
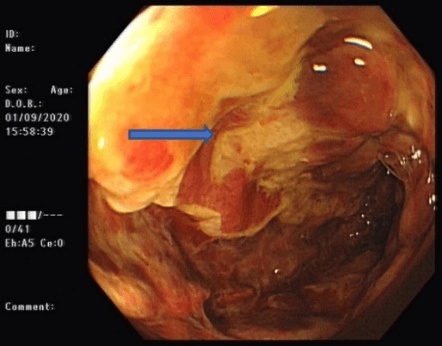
Figure 1: Endoscopic findings at index sigmoidoscopy.
Arrow: colonic stripe sign.
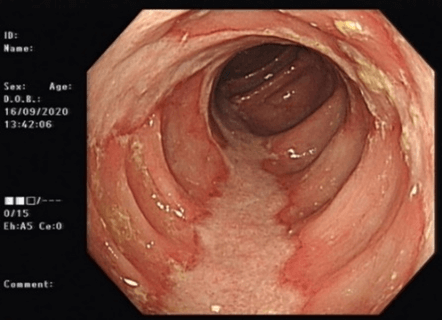
Figure 2: Endoscopic findings at interval colonoscopy.
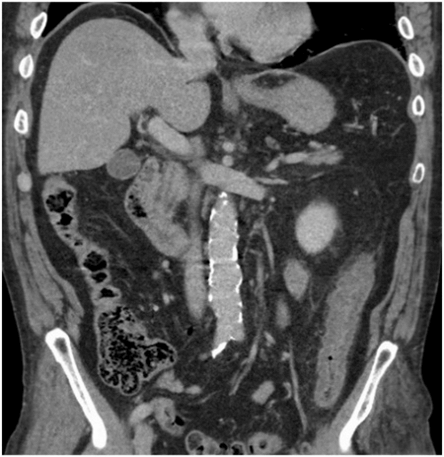
Figure 3: Coronal post-contrast abdominal CT.
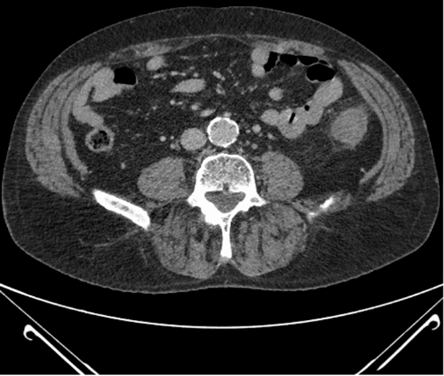
Figure 4: Axial post-contrast abdominal CT.
The histology showed fragments of fibroinflammatory material along with some normal large intestinal mucosa. In other areas, the crypts were atrophic and withered in appearance with hyalinisation of the lamina propria and variable oedema. There was surface ulceration in the descending colon. Residual crypts contained acute inflammatory debris, and there was mild superficial active inflammation. The appearances were in keeping with ischaemic colitis. Critically, there was no evidence of dysplasia or invasive malignancy in the biopsy samples sent. He was managed conservatively with fluid hydration, nil per orally, and antibiotics in the hospital. He had a good resolution of his clinical condition before discharge.
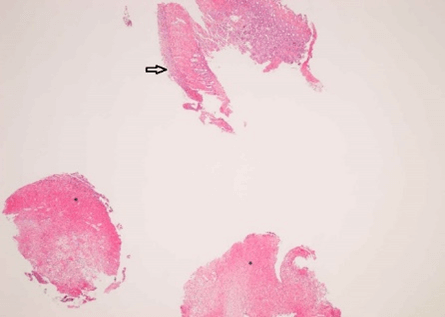
Figure 5: Descending colon (x2).
Asterisk: Fragments of inflammatory material, Arrow: Mucosal surface ulceration.

Figure 6: Descending colon (x10).
Asterisk: Atrophic crypts, Arrow: Hyalinised lamina propria.
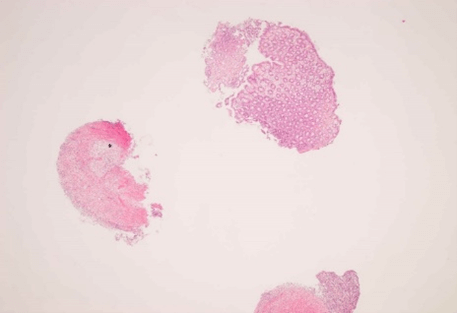
Figure 7: Splenic flexure (x2).
Asterisk: Fibroinflammatory material.
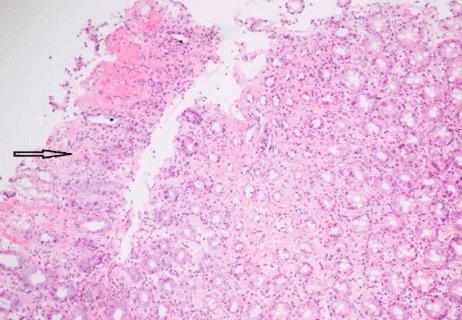
Figure 8: Splenic flexure (x10).
Asterisk: Atrophic crypts, Arrow: Hyalinised lamina propria.
Discussion
Colonic ischaemia is an uncommon vascular disease, and severe cases are associated with high mortality. Ischaemia occurs when there is insufficient perfusion to the intestinal tissue, leading to ischaemic tissue injury [1]. The most commonly affected areas for colonic ischaemia are at Griffith’s and Sudeck’s point, being anatomical “watershed areas” of vascular collateral territories, at the splenic flexure and the descending/sigmoid colon, respectively. However, all parts of the colon can be affected [2]. These areas are inherently at risk for decreased blood flow and subsequent ischaemia. Additional reperfusion injury adds to the damage caused by ischaemia [3]. The progression of mucosal injury starts with ulceration and progresses to full-thickness injury with progressive ischaemia. This mucosal injury allows translocation of bacteria, which results in bacteremia and an increased risk of sepsis. Colonic ischaemia is a challenging diagnosis to make. It has a high mortality rate, up to 50%, and the time to diagnosis and management is key to survival. Risk factors include smoking, cardiovascular disease, diabetes mellitus, chronic obstructive pulmonary disease, dyslipidemia, and atherosclerosis [4-6]. About 20% of patients with acute ischaemic colitis may develop long-term complications known as chronic ischaemic colitis [7].
The diagnosis of ischaemic colitis can be challenging, mimicking numerous other disease conditions [8, 9]. Patients can present clinically with generalized abdominal symptoms such as nausea, vomiting, diarrhoea, the passage of blood per rectum and anorexia. The more severe the underlying ischaemia, patients can present with more sinister findings, such as acute abdomen, shock or sepsis. The key to diagnosing ischaemic colitis is having a high index of suspicion and including it in the patient’s differential diagnosis. Suggestive laboratory findings include leukocytosis, metabolic acidosis, elevated amylase and elevated lactate. However, none of these is specific to colonic ischaemia. Abdominal imaging can suggest an underlying cause and help determine severity, but also be non-specific to colonic ischaemia. An endoscopy is a useful tool for the evaluation of the colon mucosa and degree of mucosal injury. It allows for histological sampling of the affected area, which is extremely useful in establishing a diagnosis [10]. The degree of mucosal injury can range from mild surface ulceration through to full-thickness gangrene/necrosis, which reflects the clinical outcome and disease severity [10].
Management of these patients is largely supportive and is dependent on the degree of mucosal injury and subsequent systemic abnormalities arising from the colonic insult. These patients may become hypotensive secondary to fluid sequestration in the bowel and loss of interstitial volume as well as sepsis from bacterial translocation. As such, these patients should be managed with aggressive fluid resuscitation and intravenous broad-spectrum antibiotics.
The differential diagnosis in these patients includes inflammatory bowel disease, acute diverticulitis, infectious colitis, solitary rectal ulcer syndrome and colorectal carcinoma. Significantly, the endoscopic features of ischaemic colitis can mimic those of colorectal carcinoma, with more extensive inflammatory masses/ulcerations appearing as neoplastic. There are multiple case reports in the literature of similar endoscopic presentations and subsequent endoscopic and histological outcomes [9, 11, 12]. This case is of particular interest because of a descending colonic mass lesion, which turned out not to be malignant.
Conclusion
It is essential to consider ischaemic colitis as a better prognosis differential for colonic masses arising at specific points of the colon in patients with relevant risk factors.
Ethics Statement
None.
Competing Interests
None.
Article Info
Article Type
Case ReportPublication history
Received: Thu 24, Sep 2020Accepted: Fri 16, Oct 2020
Published: Mon 26, Oct 2020
Copyright
© 2023 Vikrant Parihar. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.SCR.2020.10.14
Figures & Tables
Table 1: Laboratory values.
|
Laboratory values |
Values (normal range) |
|
White cell count |
16.9 x 109 cells/L (4.0-11.0) |
|
Haemoglobin |
11.6 g/dL (12.5-17.5) |
|
Mean corpuscular volume |
86.3 fL (79.0-96.0) |
|
Platelets |
280 x 109 cells/L (140-400) |
|
C-reactive protein |
55 mg/L (<5) |
|
Liver function tests |
Normal |
|
Urea, creatinine and electrolytes |
Normal |
|
Stool Culture |
Negative |
|
Clostridium difficile |
Negative |
|
Faecal calprotectin |
>6000 µg/g (<50) |
|
Lactate |
3.3 mmol/L (<2.2) |
Arrow: colonic stripe sign.
Asterisk: Fragments of inflammatory material, Arrow: Mucosal surface ulceration.
Asterisk: Atrophic crypts, Arrow: Hyalinised lamina propria.
Asterisk: Fibroinflammatory material.
Asterisk: Atrophic crypts, Arrow: Hyalinised lamina propria.
References
- Elder K, Lashner BA, Al Solaiman F (2009) Clinical approach to colonic ischaemia. Cleve Clin J Med 76: 401-409. [Crossref]
- Brandt LJ, Feuerstadt P , Blaszka MC (2010) Anatomic patterns, patient characteristics, and clinical outcomes in ischemic colitis: a study of 313 cases supported by histology. Am J Gastroenterol 105: 2245-2252. [Crossref]
- Brandt LJ, Feuerstadt P, Longstreth GF, Boley SJ, American College of Gastroenterology (2015) ACG clinical guideline: epidemiology, risk factors, patterns of presentation, diagnosis, and management of colon ischemia (CI). Am J Gastroenterol 110: 18-44. [Crossref]
- Chang L, Kahler KH, Sarawate C, Quimbo R, Kralstein J (2008) Assessment of potential risk factors associated with ischaemic colitis. Neurogastroenterol Motil 20: 36-42. [Crossref]
- Longstreth GF, Yao JF (2010) Diseases and drugs that increase risk of acute large bowel ischaemia. Clin Gastroenterol Hepatol 8: 49-54. [Crossref]
- Longstreth GF, Yao JF (2009) Epidemiology, clinical features, high-risk factors, and outcome of acute large bowel ischaemia. Clin Gastroenterol Hepatol 7: 1075-1080. [Crossref]
- Cappell MS (1998) Intestinal (mesenteric) vasculopathy. II. Ischemic colitis and chronic mesenteric ischemia. Gastroenterol Clin North Am 27: 827-860. [Crossref]
- Cerilli LA, Greenson JK (2012) The Differential Diagnosis of Colitis in Endoscopic Biopsy Specimens: A Review Article. Arch Pathol Lab Med 136: 854-864. [Crossref]
- X Zou, J Cao, Y Yao, W Liu, L Chen (2009) Endoscopic findings and clinicopathologic characteristics of ischemic colitis: a report of 85 cases. Dig Dis Sci 54: 2009-2015. [Crossref]
- Montoro MA, Brandt LJ, Santolaria S, Gomollon F, Puértolas BS et al. (2011) Clinical patterns and outcomes of ischaemic colitis: results of the Working Group for the Study of Ischaemic Colitis in Spain (CIE study). Scand J Gastroenterol 46: 236-246. [Crossref]
- Rabbanifard R, Gill JA (2014) Ischemic Colitis, the Great Imitator: A Mass Completely Resolved. ACG Case Rep J 1: 100-102. [Crossref]
- Karamouzis MV, Badra FA, Papatsoris AG (2002) A case of colonic ischemia mimicking carcinoma. Int J Gastrointest Cancer 32: 165-168. [Crossref]