Journals
Video-assisted Nuss bar insertion to stabilize a flail chest
A B S T R A C T
Surgical stabilization of flail chest decreases mortality, complications and costs. A 48-year-old male sustained a cardiac arrest followed by successful cardio-pulmonary resuscitation. An anterior flail chest due to bilateral rib fractures and a sternal fracture led to respiratory failure. A surgical stabilization of the flail chest was indicated, and a minimally invasive approach was preferred. A titanium plate for the sternum and a Nuss bar for rib fractures were successfully placed, followed by full and prompt recovery. It is an effective and safe procedure since minimizes the surgical trauma with benefits of chest wall stabilization.
K E Y W O R D S
Nuss, bar, flail, chest, stabilize, minimally invasive
Background
Surgical intervention for flail chest (FC) has been recently debated: there are evidence of outcome improvement, providing careful candidate selection and precise surgical planning [1-3]. We describe an emblematic case: the use of Nuss bar to stabilize a post traumatic FC in a patient with severe comorbidities.
Case Report
A 48-year-old male sustained a cardiac arrest in a psychiatric clinic. On site, cardio-pulmonary resuscitation was successful, the patient was intubated and admitted to Intensive Care Unit (ICU). At the time of extubation, an anterior FC was obvious, and the patient rapidly developed respiratory failure due to pain and impaired ventilator mechanism. After re-intubation, a CT scan showed bilateral rib fractures (2 to 8 on the left-hand side and 2 to 6 on the right-hand side) and a transverse sternal fracture (Figure 1). The patient had a past medical history characterized by mental disorder, hepatitis C and alcoholic liver cirrhosis Child C and drug addiction.
A surgical stabilization of the FC was indicated, and a minimally invasive approach was preferred, and the informed consent taken. As first step, sternal fixation was performed with a titanium plate (DePuy Synthes, Johnson&Johnson, Raynham, Massachusetts, US) and a Nuss bar (Pectus Support Bar System; PTY Medical Device, Shanghai, China) was then placed with video assisted thoracoscopic support to stabilize the bilateral rib fractures: two 4 cm incisions were performed bilaterally, along the fifth intercostal space. A pre-shaped still bar was passed into the pleural space under thoracoscopic monitoring. The bar was then rotated and fixed to the lateral arch of the fifth ribs with metallic sutures (Figure 2). Surgical time was 120 minutes with minimal blood loss. The patient was extubated 4 days later and recovered well. Written informed consent was obtained.
Discussion
FC is a serious condition with high mortality rate [1-3]. It leads to hypoventilation and ineffective coughing, increasing exponentially the risk of complications. Recently, several studies have shown that surgical stabilization decreases ICU stay, mortality, pulmonary complications, long term chest deformity and, ultimately costs [1-3]. Several methods and materials are available in order to choose the best surgical approach: locked plates, rib-clamp systems and intramedullary K-wires are the most commonly employed [2]. However, all of them require direct access to the fractured ribs, and when bilateral fractures occur, long or multiple incisions are needed [3]. In our case various conditions affected the surgical strategy.
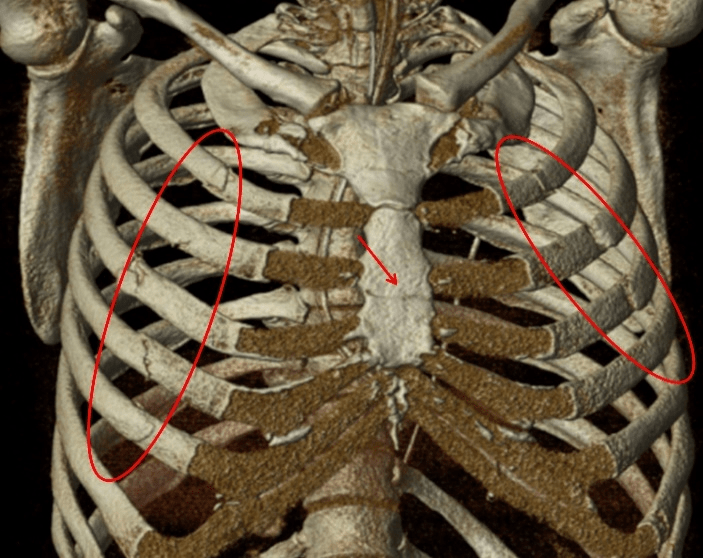
Figure 1: Volume Rendering reconstruction showing multiple bilateral rib fractures (circle) and the sternal fracture (arrow).
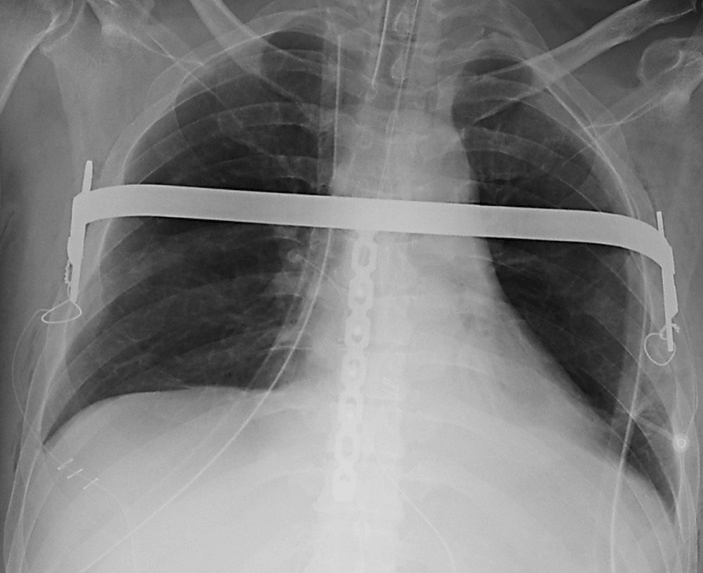
Figure 2: Chest x-ray showing the post-operative control of the Nuss bar insertion.
The coagulation disorders contraindicated the use of epidural analgesia, the history of drug addiction causes resistance to opioid painkillers and the altered mental status made the patient not compliant with respiratory physiotherapy. Besides, surgical intervention was indicated in this patient who did not have any other concomitant injuries requiring ventilator support. All the fractures involved the anterior arch of the ribs and direct access to all would have required a clamshell incision and was considered too invasive with high risk of bleeding.
The use of Nuss bar has been described in some case reports to stabilize antero-lateral FC, but in our case the sternal fracture could represent an issue because of the forces applied by the bar itself, that could separate the segments [4, 5]. To overcome this pitfall, we choose to stabilize the body of sternum as first step and sequentially proceed with the bar placement. This minimal invasive approach achieved the best result with complete stabilization of the FC, full and prompt recovery and no complications.
Conclusion
In summary, the use of video-assisted Nuss bar in this setting is a simple, effective and safe procedure; it minimizes surgical trauma and allow to extend the benefit of chest wall stabilization to those patients with relative contraindications.
Conflicts of Interest
All authors have no conflicts of interest
Funding
None
Written informed consent was obtained from the patient.The present study was conducted in accordance to the World Medical Association Declaration of Helsinki.
Article Info
Article Type
Case ReportPublication history
Received: Fri 18, Jan 2019Accepted: Tue 26, Feb 2019
Published: Sat 30, Mar 2019
Copyright
© 2023 Francesco Mongelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSR.2019.01.02
Author Info
Corresponding Author
Francesco MongelliThoracic Surgery, San Giovanni Hospital, Bellinzona, Switzerland
Figures & Tables
References
- Kocher GJ, Sharafi S, Azenha LF, Schmid RA (2017) Chest wall stabilization in ventilator-dependent traumatic flail chest patients: who benefits? Eur J Cardiothorac Surg 51: 696-701. [Crossref]
- Swart E, Laratta J, Slobogean G, Mehta S (2017) Operative Treatment of Rib Fractures in Flail Chest Injuries: A Meta-analysis and Cost-Effectiveness Analysis. J Orthop Trauma 31: 64-70. [Crossref]
- Cataneo AJ, Cataneo DC, de Oliveira FH, Arruda KA, El Dib R, et al. (2015) Surgical versus nonsurgical interventions for flail chest. Cochrane Database Syst Rev 29: CD009919. [Crossref]
- Ke S, Duan H, Cai Y, Kang J, Feng Z (2014) Thoracoscopy-assisted minimally invasive surgical stabilization of the anterolateral flail chest using Nuss bars. Ann Thorac Surg 97: 2179-2182. [Crossref]
- Murat Akkuş, Ayfer Utkusavaş, Murat Hanözü, Mehmet Kaya, Ihsan Bakir (2015) Stabilization of Flail Chest and Fractured Sternum by Minimally Invasive Repair of Pectus Excavatum. Thorac Cardiovasc Surg Rep 4: 11-13. [Crossref]