Journals
Uvula Strangulation: A Rare Case of Hair Thread Tourniquet Syndrome
A B S T R A C T
Hair thread tourniquet syndrome is a rare but previously well-documented presentation. It is described as circumferential strangulation of distal or multiple distal appendages, which can lead to tissue ischaemia and eventually necrosis without prompt treatment. Despite the characteristic presentation and potential for serious complications, many healthcare professionals remain unaware of hair tourniquet syndrome and the need for urgent management. We present the case of a 9-month-old infant who presented to the emergency department. The parent noted a long hair emanating from the mouth but on attempts to remove it was unable to do so. The child was otherwise stable. Examination on the oral cavity revealed the hair strand tightly wrapped around an oedematous and congested uvula. Attempts to remove the ligature in the emergency department were unsuccessful and a subsequent referral to otolaryngology was made. A decision was made to take the child to the operating theatre, where the ligature was successfully removed with the distal uvula remaining viable.
Keywords
Hair thread tourniquet syndrome, uvula ischaemia, management of hair tourniquet, syndrome
Introduction
Hair thread tourniquet syndrome is a rare but previously well-documented presentation. It was first described in 1612 by Guillemeau and first appeared in the literature in The Lancet in 1832 [1]. It has multiple pseudonyms such as hair wrapping, hair tourniquet, and hair thread constriction but the term hair thread tourniquet syndrome was first used by Barton et al. in 1988 [1, 2-4]. Hair thread tourniquet syndrome is described as when hair (or textile thread) wraps around one or multiple distal appendage/s with an end arterial supply, acting as a ligature causing partial or total circulation loss to the distal part. This, in turn, leads to ischaemia, necrosis, and loss of distal appendages with associated complications unless prompt management is undertaken [4, 5].
Circumferential constriction of the appendage causes distal swelling and erythema with associated pain. The presentation can be acute or subacute, sometimes presenting after several days. The hair can cut through the epithelium and re-epithelialisation over the hair may occur, making visualization of the hair and therefore, diagnosis surprisingly difficult [5]. The basis of the management is the removal of the tightly bound hair and this can be done by unwrapping, cutting or dissolving the offending fibre, and return of circulation [3, 6]. As such, this should be treated as an avascular emergency however, it is frequently overlooked or mismanaged.
Hair thread tourniquet syndrome can present with a tourniquet of any distal appendage but most commonly affects penis, toes, fingers, other sites (clitoris, labia majora). It rarely affects the head and neck region with just two cases of tourniquet of the uvula and two cases of tourniquet of the neck described in the literature [7]. Commonly it presents in children under five and there are occasional reports in older children and adults, although in these cases, there is usually concomitant impairment of cognition [7-9].
Case Presentation
We present the case of a 9-month-old infant who presented to the emergency department. The parent noted a long hair emanating from the mouth but on attempts to remove it was unable to do so. The child was otherwise clinically stable. Examination on the oral cavity revealed the hair strand tightly wrapped around an oedematous, congested uvula with no necrosis (Figure 1). Attempts to remove the ligature in the emergency department were unsuccessful and a subsequent referral to otolaryngology was made. A decision was made to take the child to the operating theatre urgently (within 1 hour), where the ligature was successfully removed (Figure 2). The distal uvula remained healthy and viable, and the child had an uneventful postoperative recovery. Follow-up revealed a normal-appearing uvula.
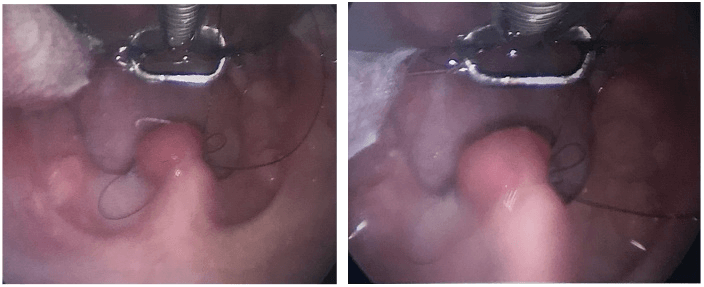
Figure 1: Oral cavity (Boyle-Davis mouth gag in situ). Hair ligature wrapped tightly around an oedematous uvula, with distal congestion.
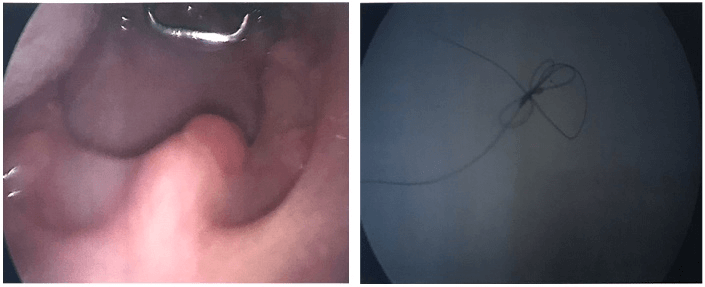
Figure 2: Oral cavity (Boyle-Davis mouth gag in situ). Hair ligature removed, with the viable distal uvula.
Discussion
Whilst ‘hair thread tourniquet syndrome’ has been frequently described in the literature in relation to tourniquet of the toes, fingers and genitals, there are only two documented cases of uvula tourniquet. Krishna et al. described a case in 2002 with a similar presentation to our case and removed the hair tourniquet under general anaesthetic with the survival of the uvula [10]. Mcneal et al. in 1987 described a case of uvula hair tourniquet. They failed to remove the ligature while the child was conscious, and it was felt not in the child’s best interest to undergo a general anaesthetic. The child was discharged and reviewed 48 hours later by which time the distal tip of the uvula had self-amputated. They stated although this was sub-optimal, there were no long-lasting sequelae from the loss of the distal uvula [2].
The complications resulting from ischaemia due to occlusion of vasculature in distal appendages with end arterial supply are obvious and include partial amputation, complete amputation, and deformity [7]. These complications in regard to cases of genital or digit hair tourniquets are severe and life-changing, the long-term impact of autoamputation of the uvula is less dramatic but any preventable loss of functional tissue should be seen as sub-optimal. There is also the potential for aspiration of a self-amputated uvula and associated complications.
Therefore, patients presenting with symptoms characteristic of ‘hair thread tourniquet syndrome’ should have prompt specialty review and removal of the hair tourniquet, either by using simple measures such as unwinding or if these fail by surgical intervention [6]. The sooner the successful removal of the hair tourniquet, the lower the chance of tissue damage occurring and loss of function.
Article Info
Article Type
Case ReportPublication history
Received: Mon 10, Aug 2020Accepted: Mon 24, Aug 2020
Published: Fri 04, Sep 2020
Copyright
© 2023 Joseph Stansfield. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.IJSCR.2020.03.10
Author Info
Corresponding Author
Joseph StansfieldENT Department, Royal Manchester Children’s Hospital, Manchester, United Kingdom
Figures & Tables
References
- M F Abel, R McFarland 3rd (1993) Hair and Thread Constriction of the Digits in Infants. J Bone Joint Surg Am 75: 915-916. [Crossref]
- R M McNeal, J C Cruickshank (1987) Strangulation of the Uvula by Hair Wrapping. Clin Pediatr (Phila) 26: 599-600. [Crossref]
- Aisling O'Gorman, Savithiri Ratnapalan (2011) Hair Tourniquet Management: Pediatr Emerg Care 27: 203-204. [Crossref]
- D J Barton, G M Sloan, L S Nichter, J F Reinisch (1988) Hair-Thread Tourniquet Syndrome. Pediatrics 82: 925-928. [Crossref]
- Niroshan Sivathasan, Lavnya Vijayarajan (2012) Hair-Thread Tourniquet Syndrome: A Case Report and Literature Review. Case Rep Med 2012: 171368. [Crossref]
- Jonathan F Bean, Ferdynand Hebal, Catherine J Hunter (2015) A single center retrospective review of hair tourniquet syndrome and a proposed treatment algorithm. J Pediatr Surg 50: 1583-1585. [Crossref]
- Arman Z Mat Saad, Elizabeth M Purcell, Jack J McCann (2006) Hair-Thread Tourniquet Syndrome in an Infant with Bony Erosion: A Case Report, Literature Review, and Meta-analysis. Ann Plast Surg 57: 447-452. [Crossref]
- Ram R Miller, William E Baker, Gary H Brandeis (2004) Hair-Thread Tourniquet Syndrome in a Cognitively Impaired Nursing Home Resident. Adv Skin Wound Care 17: 351-352. [Crossref]
- FS Haddad (1982) Penile Strangulation by Human Hair. Report of three cases and review of the literature. Urol Int 37: 375-388. [Crossref]
- Sangeeta Krishna, Ronald I Paul (2003) Hair tourniquet of the uvula. J Emerg Med 24: 325-326. [Crossref]