Unusual Post-Traumatic Under-Serosa Rupture of the Gallbladder
A B S T R A C T
Gallbladder lesions due to blunt abdominal injury are rare, being found in only about 2% of patients who undergo laparotomy for abdominal trauma. It is commonly associated with other concomitant visceral injuries. It is challenging to make an early diagnosis. We report the case of a 35-year-old woman victim of a public road accident who underwent laparotomic cholecystectomy. Acute post traumatic cholecystitis was suspected based on clinical and radiologic data. Perioperative findings showed no ascites, but a distended gallbladder. Its serosa was intact. After its removal, we opened the gallbladder, we discovered a rupture of the mucosa and bile trapped between the mucosa and the serosa of the gallbladder. The postoperative course was simple.
Keywords
Cholecystectomy, gallbladder rupture, trauma
Introduction
Traumatic gallbladder rupture occurs rarely after blunt abdominal injuries [1, 2]. This small organ is protected by surrounding organs including the liver, intestines, omentum, and ribs [1]. It is often associated to injury of other organs. Gallbladder rupture usually include continuity solution of all its layers responsible for a bile issue in the abdominal cavity. Diagnosis of gallbladder rupture is difficult due to the lack of specific symptoms [1]. It is challenging to detect a defect in the gallbladder wall even when using imaging such as ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI) [2]. We report an exceptional case of under serosa rupture of the gallbladder after blunt abdominal trauma.
Case Report
35-year-old patient, with no previous history, was a victim of a road accident. Pedestrian hit by a car. On admission to our emergency department, her vital signs were stable. Physical examination revealed tenderness of the right upper quadrant. Complete blood count revealed slightly elevated white blood cells of 11250/mm3, elevated liver enzymes AST of 152 U/L, ALT of 267 U/L and cholestasis of twice normal. the rest of the biological assessment was normal. The abdominal ultrasound showed a distended gallbladder to 13 cm. Abdominal CT (Figure 1) revealed distension of the gallbladder to 14 cm with significant edema. The two exams showed a low abundance intraperitoneal liquid and no lesion of other organs. The patient was operated. A median laparotomy was performed. Exploration found a distended gallbladder with rupture of the gallbladder wall. However, bile was trapped by the peritoneal covering of the gallbladder (Figure 2). Intraoperative cholangiography did not show damage to the biliary ducts. Cholecystectomy revealed a 3mm wound beneath the serosa of the infundibulum of the gallbladder (Figure 3). The postoperative course was simple.
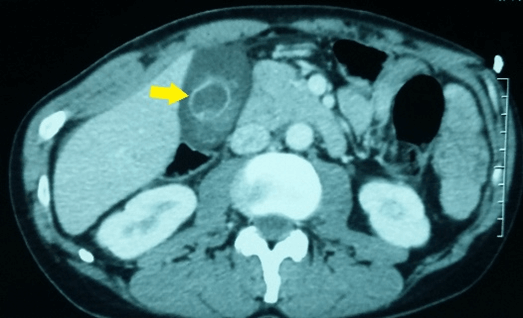
Figure 1: CT scan findings. Arrow: distension and edema of the gallbladder.
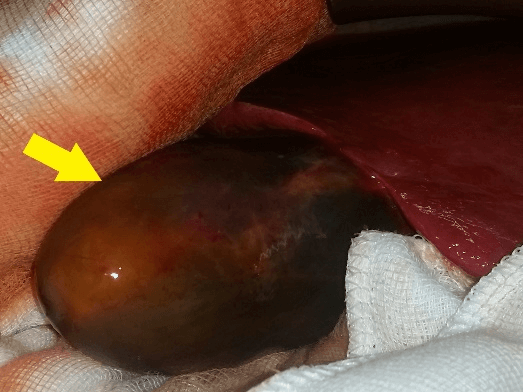
Figure 2: Preoperative findings. Arrow: bile trapped under gallbladder serosa.
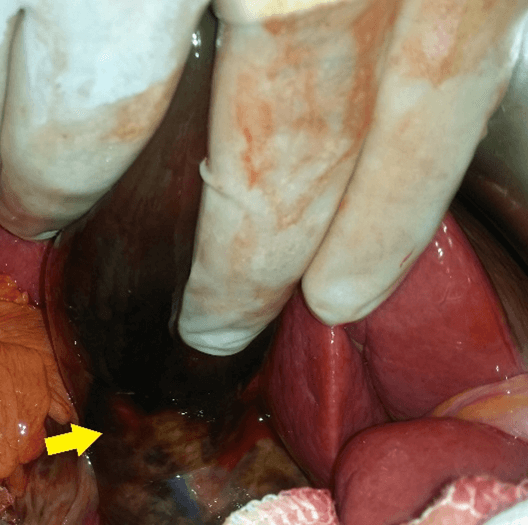
Figure 3: Gallbladder injury. Arrow: infundibular under serosa rupture.
Discussion
Gallbladder injury resulting from blunt abdominal trauma exceptional [1, 2]. Its deep location and its small size provide good protection. Gallbladder injuries are found in only about 2% of patients who undergo laparotomy for abdominal trauma [2]. Isolated gallbladder injury, as in this case, is even rarer. Risk factors to gallbladder injury include a thin-walled gallbladder, a distended gallbladder, and alcohol ingestion [2, 3]. Review of the literature found that gallbladder injuries can be classified as contusion, perforation, or avulsion [2-5]. Contusion is defined as an intramural hematoma. Perforation is the most common gallbladder injury reported. It is associated with choleperitoneum. The most severe injury, gallbladder avulsion, can be further stratified by degree of tearing from the liver. In partial avulsion, the gallbladder is partially detached from the liver bed. In complete avulsion, the gallbladder is completely detached from the liver bed, but the cystic duct and artery remain intact [5]. Total avulsion is when the gallbladder is free in the abdomen without any attachments [5].
Diagnosis of gallbladder injury is difficult especially when it is isolated [4]. It is often established during surgical exploration. Patients with isolated gallbladder injuries present nonspecific and delayed symptoms [1, 2, 4]. In the period shortly after trauma, the leakage of bile does not irritate the peritoneum to be responsible of signs of acute peritonitis [4]. In our case, bile was trapped under the serosa. Laboratory tests may often be normal [1]. Abdominal ultrasound and CT are the most contributing imaging examinations [2, 4, 6]. CT appears to be the most effective. The diagnosis can be made by detection of blood in the gallbladder lumen. High-density fluid within the lumen, thickening or indistinctiveness of the gallbladder wall, and active arterial extravasation into the lumen suggest gallbladder injury [3, 6].
Treatment is dependent on the type and severity of injury. For gallbladder contusions or small lacerations, an expectant attitude consisting in medical treatment with possibly radiological drainage can be adopted [1, 2, 5, 7]. For more severe injury cholecystectomy is recommended. Laparoscopic approach is the gold standard. Because of the rarity of isolated gallbladder injury, prognosis is not well known. Most authors found that, when diagnosed early, the prognosis is quite good [1-3]. It depends mainly on the precocity of diagnosis and the concomitant organs injury.
Conclusion
Isolated gallbladder injury after blunt abdominal trauma is exceptional. Diagnosis can be challenging. Patients have no specific clinical presentation. CT appears to be the most contributive radiologic exploration. Treatment consists in cholecystectomy in severe cases. Prognosis is dominated by the association with other organ injuries and early diagnosis.
Acknowledgment
None.
Conflicts of Interest
None.
Article Info
Article Type
Case ReportPublication history
Received: Mon 07, Jun 2021Accepted: Tue 03, Aug 2021
Published: Thu 19, Aug 2021
Copyright
© 2023 Guizani Rami. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.GSCR.2021.02.01
Figures & Tables
References
1.
Soderstrom CA,
Maekawa K, Dupriest RW, Cowley RA (1981) Gallbladder Injuries Resulting from
Blunt Abdominal Trauma: An Experience and Review. Ann Surg 193: 60-66. [Crossref]
2.
Kwan BYM,
Plantinga P, Ross I (2015) Isolated traumatic rupture of the gallbladder. Radiol
Case Rep 10: 1029. [Crossref]
3.
Pavlidis TE,
Lalountas MA, Psarras K, Symeonidis NG, Tsitlakidis A et al. (2011) Isolated
complete avulsion of the gallbladder (near traumatic cholecystectomy): a case
report and review of the literature. J Med Case Rep 5: 392. [Crossref]
4.
Birn J, Jung M,
Dearing M (2012) Isolated gallbladder injury in a case of blunt abdominal
trauma. J Radiol Case Rep 6: 25-30. [Crossref]
5.
Ball CG, Dixon E,
Kirkpatrick AW, Sutherland FR, Laupland KB et al. (2010) A decade of experience
with injuries to the gallbladder. J Trauma Manag Outcomes 4: 3. [Crossref]
6. Jaggard MKJ, Johal NS, Choudhry M (2011) Blunt abdominal trauma resulting in gallbladder injury: a review with emphasis on pediatrics. J Trauma 70: 1005-1010. [Crossref]
7. Wittenberg A, Minotti AJ (2005) CT diagnosis of traumatic gallbladder injury. AJR Am J Roentgenol 185: 1573-1574. [Crossref]