Unusual Case of Acetabular Liner Dissociation Following Failure of Ceramic-OnCeramic Bearing Total Hip Arthroplasty: A Case Report
A B S T R A C T
Modular hip implants can improve construct stability and the rate of volumetric wear in Total Hip Arthroplasty (THA), however, there is still a 0.2-10% risk of dislocation. We report the unusual case of a 54-year-old lady who presented with a dislocated migrated ceramic liner following a twisting injury. She had undergone a ceramic-on-ceramic THA five years earlier. This diagnosis of the dislocated liner was confirmed with computed tomography (CT) scanning. Review of National Joint Registry data showed ceramic-on-ceramic acetabular liner dissociation to be rarer than in those with metal-on-polyethylene (incidence 0.27 vs. 0.46 per 1000 prosthesis years). We suggest the liner may have migrated in retrograde along the iliopsoas. We recommend the use of cross-sectional imaging (CT) to assist in confirming the diagnosis and planning future surgery.
Keywords
Ceramic liner, dislocation, migration, computed tomography
Introduction
Modern Total Hip Arthroplasty (THA) tend to be modular in design. Modular hip implants provide an additional interface between the prosthetic head and the outer shell. This design allows you to change the effective head diameter and level of constraint in total hip arthroplasty which may, in turn, be beneficial by changing the rate of volumetric wear and improving stability respectively [1, 2]. Modularity allows a greater number of component combinations that can be tailored to the clinical needs and the patients’ expectations, as well as the ability to exchange modular components in wear, infection, or recurrent dislocation [3]. Dislocation following THA ranges from 0.2-10% per year and patients must be consented for this pre-operatively [4, 5].
Case Presentation
Situation
Patient MA, a 54-year-old female, attended the emergency department with left hip pain after twisting whilst loading her left leg. She described a sudden discomfort and a crunching sensation. She had undergone a left Exeter/Tritanium ceramic-on-ceramic total hip replacement 5 years before this for avascular necrosis of the left hip. Initial radiographs of the pelvis and hips demonstrated bilateral total hip replacements in situ. On the anteroposterior radiograph, it was noted that the femoral head was not centred within the acetabular component, in keeping with asymmetric wear (Figure 1). The patient had ongoing pain and re-presented to the emergency department 10 days later with a clunking sensation. Further radiographs confirmed that the femoral head was located within the acetabular component but was maintained in an eccentric position (Figure 2). Due to persistent symptoms, the patient was referred to a hip surgeon. Review of the previous radiographs taken in the emergency department revealed that there was an opacity seen in the left hemipelvis overlying the left ilium. The diagnosis of a dislocated ceramic liner was confirmed on computed tomography (CT) scanning (Figure 3). The patient was informed of this and placed on the urgent list for revision hip surgery.
During the revision surgery, the ceramic femoral head was seen lying in the metal acetabular component. The ceramic acetabular liner was not seen, nor was there any evidence of ceramic debris. The liner and head were changed to a Stryker dual-mobility construct. The patient made an uneventful postoperative recovery and reported no problems with the dislocated migrated ceramic liner retained within the pelvis (Figure 4).
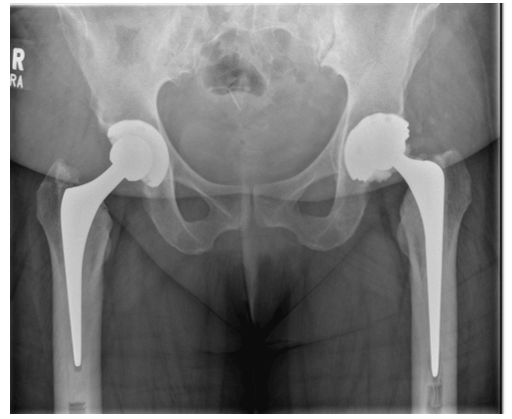
Figure 1: AP radiograph pelvis.
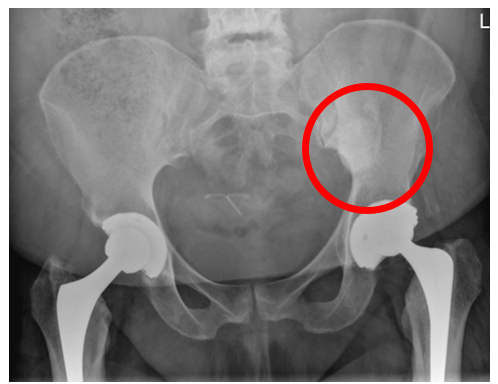
Figure 2: AP radiograph pelvis showing opacity over left iliac blade and non-concentric position of femoral head within the acetabular component.

Figure 3: Axial CT radiographs. The dissociated component is ringed in red.

Figure 4: Post operative radiograph after revision hip surgery.
Discussion
In 2018, 27, 605 (2.8%) of the 992,090 primary hip replacements had an associated first revision. A review of ten-year National Joint Registry (NJR) data shows an acetabular liner dissociation incidence of 0.27 per 1000 prosthesis years in uncemented ceramic-on-ceramic hips compared to 0.46 in metal-on-polyethylene [6].
Dissociation of liner components is uncommon, and migration of the liner is rarely cited. In previous cases of persistent hip pain following dislocation, CT and MRI imaging has shown that polyethylene hip liners can migrate to the soft tissues of the posterior thigh, and between the gluteus medius and minimus [7, 8]. Failure of the locking mechanism between the liner and the shell appears to be a common cause for failure and dissociation of these hips [3, 9]. Ceramics are more often associated with catastrophic failure and fragmentation of the liner, usually found within the acetabular shell in the surrounding soft tissues during revision [10]. In a systematic review performed by Traina et al. it was suggested that adjunctive CT scan be performed to refine the diagnosis and better characterise the mutual relationship between the cup and the stem in ceramic hips [11].
In this particular case, the ceramic liner had dissociated itself from the metal-backed liner and had migrated superiorly into the pelvis. This has not been described before in the literature and we suggest that it might have taken the route along the iliopsoas in a retrograde manner or posteriorly along the piriformis via the greater sciatic notch.
Message
It is important to suspect liner dissociation as a cause of sudden pain associated with a crunching sensation. Plain radiographs of the whole pelvis may reveal signs of potential liner dissociation usually around the hip and the surrounding soft tissues. However, very occasionally the liner may migrate further afield and, in these circumstances, cross-sectional imaging, namely computed tomography can be very helpful to confirm the diagnosis and plan further surgery.
Article Info
Article Type
Case ReportPublication history
Received: Tue 02, Jun 2020Accepted: Mon 15, Jun 2020
Published: Mon 29, Jun 2020
Copyright
© 2023 Mehool Acharya. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSCR.2020.03.07
Figures & Tables
References
- Guyen O, Pibarot V, Vaz G, Chevillotte C, Béjui Hugues J (2008) Use of a dual mobility socket to manage total hip arthroplasty instability. Clin Orthop Relat R 467: 465-472. [Crossref]
- Rhyu KH, Bae CI, Nam JH, Bae JG, Cho YJ et al. (2017) Dissociation of Polyethylene Liner of the Dual Mobility Acetabular Component after Closed Reduction of Dislocation: A Case Report. Hip Pelvis 29: 133-138. [Crossref]
- O’Neill CKJ, Napier RJ, Diamond OJ, O’Brien S, Beverland DE (2015) Acetabular Liner Dissociation following Total Hip Arthroplasty: A Rare but Serious Complication That May Be Easily Misinterpreted in the Emergency Department. Case Reports Emerg Medicine 2015: 802753. [Crossref]
- Dargel J, Oppermann J, Brüggemann GP, Eysel P (2014) Dislocation following total hip replacement. Deutsches Ärzteblatt Int 111: 884-890. [Crossref]
- Meek RMD, Allan DB, McPhillips G, Kerr L, Howie CR (2006) Epidemiology of Dislocation after Total Hip Arthroplasty. Clin Orthop Relat Res 447: 9-18. [Crossref]
- Man NJR for EWNI and the I of. 15th Annual Report 2018. 220.
- Delaney F (2017) An unusual complication of hip dislocation after total hip replacement.
- Banka TR, Ast MP, Parks ML (2014) Early Intraprosthetic Dislocation in a Revision Dual-mobility Hip Prosthesis. Orthopedics 37: e395-e397. [Crossref]
- Yamamoto K, Shishido T, Tateiwa T, Katori Y, Masaoka T et al. (2004) Failure of ceramic THR with liner dislocation - a case report. Acta Orthop Scand 75: 500-502. [Crossref]
- Hwang SK, Oh JR, Her MS, Shim YJ, Cho TY et al. (2008) Fracture-dissociation of ceramic liner. Orthopedics 31: 804. [Crossref]
- Traina F, Fine MD, Martino AD, Faldini C (2013) Fracture of ceramic bearing surfaces following total hip replacement: a systematic review. Biomed Res Int 2013: 157247. [Crossref]
- Jang JH, Jin W, Chun YS, Rhyu KH, Park SY et al. (2014) The tram track sign: a characteristic sonographic feature of polyethylene liner dissociation after total-hip arthroplasty. J Ultrasound Med 33: 1931-1937. [Crossref]