Twist without a Turn: A Rare Case Report of Mal-Rotated Gut with Caecal and Ascending Colon Volvulus in an Adult
A B S T R A C T
Midgut malrotation is a pathology seen in approximately 1:500 live births. It is an anomaly of fetal intestinal rotation that usually presents in the first month of life. It is rare for malrotation to present in adulthood. Symptomatic patients present either acutely with intestinal obstruction and ischemia with a midgut or caecal volvulus, or chronically with vague abdominal pain. In adult life, it is mostly diagnosed incidentally during a radiological investigation or during surgery for an unrelated condition as it is generally asymptomatic in adults. We present a rare case of a patient who presented to us with obstruction due to a mal-rotated gut with caecal and ascending colon volvulus with Ladd’s bands and was operated in our institution.
Keywords
Volvulus of midgut, intestinal obstruction, adult, abdominal pain, ischemia
Introduction
Midgut malrotation is a condition that is seen in approximately 1:500 live births due to abnormal rotation of the gut during intrauterine life [1, 2]. It is generally seen in children but can present in adolescents and adults too. In such a case, the presentation may vary [3]. The diagnosis is mostly established by the end of the first year of life. If it is diagnosed in adult life, it is mostly diagnosed incidentally during a radiological investigation or during surgery for an unrelated condition. This is because, in adults, it is mostly asymptomatic [4]. One of the dreaded complications of intestinal malrotation is volvulus which is characterized by bowel twisting on its mesentery thereby causing compression of blood vessels supplying the bowel [5]. It is characterized by bilious vomiting, recurrent abdominal pain, distension and in cases of infarction, shock and peritonitis [1]. We present a rare case of acute intestinal obstruction due to caecal and ascending colon volvulus due to malrotation of midgut.
Case Presentation
A 20-year-old gentleman presented to the surgical emergency with chief complaints of abdominal pain for the last 2 days and obstipation for the last 2 days. The pain was sudden in onset, localized to the left lower side of the abdomen, gradually progressive, continuous, and sharp. There was a history of diarrhoea 5 days before the day of presentation which resolved in 2 days and was associated with on and off undocumented fever episodes with chills for the last 10 days. There was no history of vomiting, weight loss, per-rectal bleeding, or melena. There were no known comorbidities.
On general physical examination, the patient was conscious and afebrile with a blood pressure of 126/82 mmHg and a pulse rate of 70/min. The abdomen was soft with no distension. There was tenderness in the left lower quadrant on palpation with no guarding or rigidity and bowel sounds were exaggerated on auscultation. On DRE, there was no faecal staining present. The blood investigations were within normal limits. Abdominal x-ray (Figure 1) revealed dilated large bowel loop with a single air-fluid level which was suggestive of obstruction. On ultrasonography of the abdomen, there was the presence of dilated bowel loops on the left side of the abdomen indicating obstruction. The mesenteric nodes were found to be enlarged with the largest one measuring approximately 12mm. A provisional diagnosis of colitis with closed-loop obstruction was made. A CECT abdomen was done to aid in the diagnosis which revealed (Figures 2-4) gross dilatation of large bowel loops on the left side of the abdomen with twisting of mesentery seen inferomedial to it giving a whirlpool appearance suggestive of volvulus involving caecum and ascending colon. The duodenojejunal flexure was seen anterior to the descending aorta with small bowel loops on the right side and large bowel loops on the left side of the abdomen with superior mesenteric vein anterior and towards the left of superior mesenteric artery suggestive of midgut malrotation. A final diagnosis of malrotation of the midgut with caecal and ascending colon volvulus leading to intestinal obstruction was made.

Figure 1: X-ray abdomen (erect and supine) showing single air fluid level (asterisk) and dilated large bowel loops(arrow) respectively.
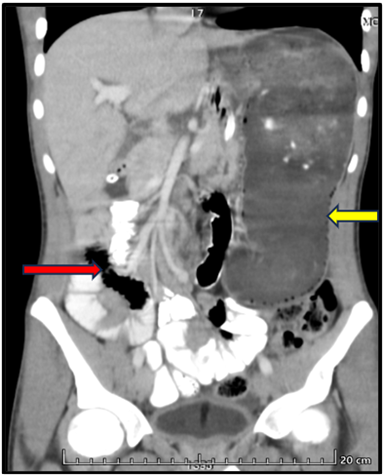
Figure 2: CECT whole abdomen (coronal section) showing dilated large bowel loops present on left side (yellow arrow) and the small bowel loops present on the right side of the abdomen (red arrow).
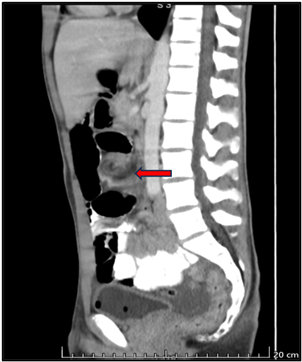
Figure 3: CECT whole abdomen (sagittal section) showing twisting of the mesentery with whirlpool appearance (red arrow) suggestive of midgut volvulus.
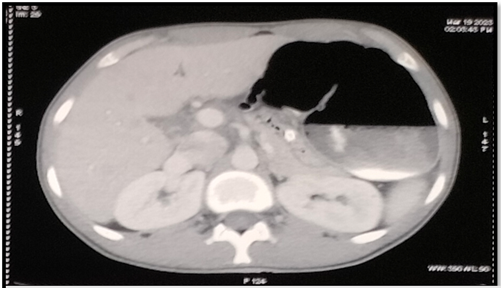
Figure 4: CECT whole abdomen (transverse section) showing dilated large bowel loops on the left side of abdomen with superior mesenteric vein present on left and anterior to superior mesenteric artery.
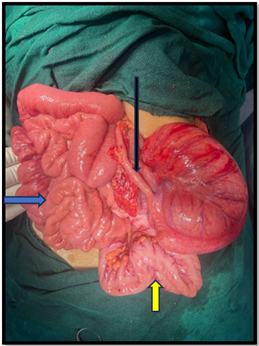
Figure 5: Intra operative picture showing entire small bowel loops present on right side (blue arrow), caecum and ascending colon on left side of abdomen with long and healthy appendix (black arrow), collapsed transverse colon (yellow arrow).

Figure 6: Intra operative picture showing massively dilated caecum and ascending colon (green arrow) present on the left side of abdomen.
The patient was taken up for emergency exploratory laparotomy. Intraoperatively Ladd’s bands were encountered which were excised. Whole of the small bowel loops were present on the right side of the abdomen. Caecum, appendix, and ascending colon were present in the left upper abdomen with volvulus involving the caecum and ascending colon. The caecum and ascending colon were massively dilated with collapsed transverse, descending, and sigmoid colon suggesting that the obstruction was at the level of ascending colon (Figures 5 and 6). The appendix was long and healthy. The mesocolon of descending and sigmoid colon were found to be redundant. On derotation of the volvulus, there was restoration of the blood supply of the caecum and ascending colon as suggested by return of normal colour and peristalsis. Other part of large intestine and small intestine appeared healthy. Multiple enlarged mesenteric lymph nodes were present with a maximum size of 3 cm. An appendicectomy with sutured caecopexy was done to fix the mobile caecum to the parietal wall.
Discussion
Adults rarely present with symptomatic midgut malrotation at first. When imaging tests are performed for other symptoms in adults or when surgery is performed for an unrelated condition, malrotation may be encountered an incidental diagnosis. It is much more common in children who are generally symptomatic [4].
Any variation from the typical 270-degree anticlockwise rotation of the intestine during embryonic development is called midgut malrotation. Normal rotation of the gut starts in the 4th week of intra uterine life (IUL) and involves the characterization of the gut tube into the foregut, midgut, and hindgut according to the anatomical blood supply. At around the 6th week of IUL, there is a brief physiological herniation of bowel, which returns to the abdominal cavity 4 to 6 weeks later. The 10th week of embryonic development marks the beginning of the gradual reduction of the physiological midgut herniation and placement of abdominal organs in their respective final anatomical positions [1].
In adults, malrotation generally is asymptomatic. Even when there are symptoms, they are non-specific and hence do not aid much in the diagnosis [6]. In our case, the patient presented with obstipation and abdominal pain which are non-specific symptoms. The history of fever was also non-specific in our patient. According to Emanuva et al. intestinal obstruction is seen because the Ladd’s bands compress the hollow organs thereby causing symptoms of obstruction [4]. In our case, ascending colon volvulus was also seen. According to Moldrem et al. volvulus occurs when the last stage of rotation that is the colonic rotation is impaired [7].
Due to the non-specificity of the clinical presentation, radiological investigations are most useful to make the diagnosis. In the case of adults, a CT scan of the abdomen is the preferred investigation which shows characteristic findings in a case of volvulus [8]. On ultrasound Doppler and CECT, a characteristic whirlpool sign is seen which is due to twisted mesentery and fixed midline bowel along the SMA axis, together with duodenal dilatation and distal tapering [1, 9]. Our case also had a similar finding (Figure 3).
As this was a symptomatic case of malrotation of the intestine with volvulus, surgical management was the mainstay of management. The cause of intestinal obstruction was the Ladd’s bands which were excised during the exploratory laparotomy. These bands extend from the right hypochondrium under the liver to the cecum compressing the duodenum from outside causing symptoms of obstruction with bilious vomiting. This is known as Ladd’s procedure classically described by Dr. Wiliam Ladd in the 1930s [10].
Conclusion
To summarise, malrotation in adults is rare and often an incidental finding. Prompt diagnosis is essential to avoid complications due to a compressed superior mesenteric artery. In such cases, appropriate radiological investigations should be ordered and an urgent surgical intervention must be undertaken. Fixation of mobile parts of gut is essential to preserve recurrence of volvulus. During our literature search with keywords ‘Gut malrotation’ and ‘caecal volvulus’ on PUBMED, 9 results were found out of which only 1 had both which makes it a rare case.
Article Info
Article Type
Case ReportPublication history
Received: Wed 27, Sep 2023Accepted: Thu 12, Oct 2023
Published: Mon 23, Oct 2023
Copyright
© 2023 Anubhav Vindal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2023.03.03
Figures & Tables
References
1.
Torres AM, Ziegler
MM (1993) Malrotation of the intestine. World J Surg 17: 326-331. [Crossref]
2.
Maxson RT, Franklin
PA, Wagner CW (1995) Malrotation in the older child: surgical management,
treatment, and outcome. Am Surg 61: 135-138. [Crossref]
3.
Fischer JE, Bland
KI (2007) Mastery of surgery. 5th edition. Philadelphia: Lippincott
Williams & Wilkins.
4.
Emanuwa OF,
Ayantunde AA, Davies TW (2011) Midgut malrotation first presenting as acute
bowel obstruction in adulthood: a case report and literature review. World J
Emerg Surg 6: 22. [Crossref]
5.
Pelucio M, Haywood
Y (1994) Midgut volvulus: An unusual case of adolescent abdominal pain. Am J
Emerg Med 12: 167-171. [Crossref]
6.
Wang CA, Welch CE
(1963) Anomalies of intestinal rotation in adolescents and adults. Surgery
54: 839-855. [Crossref]
7.
Moldrem AW,
Papaconstantinou H, Broker H, Megison S, Jeyarajah DR (2008) Late presentation
of intestinal malrotation: an argument for elective repair. World J Surg
32: 1426-1431. [Crossref]
8.
Pickhardt PJ,
Bhalla S (2002) Intestinal Malrotation in Adolescents and Adults: Spectrum of
Clinical and Imaging Features. AJR Am J Roentgenol 179: 1429-1435. [Crossref]
9. Pracros JP, Sann L, Genin G, Tran-Minh VA, Morin de Finfe CH et al. Ultrasound diagnosis of midgut volvulus: the "whirlpool" sign. Pediatr Radiol 22: 18-20. [Crossref]
10. Ladd WE (1936) Surgical diseases of the alimentary tract in infants. N Engl J Med 215: 705-708.