Twist of a Lifetime: A Transverse Colon Volvulus
A B S T R A C T
Transverse colon volvulus is a rare but serious cause of large bowel obstruction, often necessitating urgent surgical intervention to prevent complications such as strangulation and perforation. We present a case of a 55-year-old man who presented with a one-day history of abdominal symptoms. Emergency abdominal computed tomography (CT) revealed transverse colon volvulus, leading to immediate laparotomy and successful detorsion with resection of the affected segment. Postoperative recovery was uneventful, and the patient was discharged in stable condition. This case underscores the importance of prompt diagnosis through imaging, particularly CT, in guiding appropriate therapeutic measures. Additionally, the discussion highlights the rarity of transverse colon involvement, predisposing factors, clinical presentations, and the necessity of surgical intervention, emphasizing the higher mortality rate associated with delayed diagnosis.
Keywords
Transverse colon, volvulus, management, spontaneous
Introduction
Transverse colon volvulus is an uncommon cause of large bowel obstruction. It usually presents as a surgical emergency as acute intestinal obstruction, strangulation, and perforation peritonitis if not diagnosed early. Abdominal computed tomography (CT), performed on an emergency basis, can help to diagnose this obstruction before surgery and help in the selection of a therapeutic approach [1]. We report a rare case of transverse colon volvulus patient who was managed successfully at our institution.
Case Presentation
A 55-year-old man presented to general surgery emergency with a 1-day history of non- passage of feces and flatus, generalized pain abdomen, progressive abdominal distension, nausea and vomiting. There was no significant past medical history, no history of chronic constipation, psychiatric disease, or abdominal surgery. There was no history of any co-morbidity.
On examination, the patient was afebrile, pulse 86/minute, respiratory rate 23/minute, and blood pressure 148/90 mmHg. On per abdomen examination there was distension of abdomen without any signs of peritonitis. His abdomen was tympanic to percussion, all hernia orifices were normal. A digital rectal examination revealed an empty rectal vault without any intraluminal mass. Abdomen x ray revealed extreme dilatation of large bowel loops occupying majority of the abdomen with no air fluid level (Figure 1).
His blood investigations were as follows, haemoglobin-10.7g/dL, TLC 5100/uL, DLC-80/18 platelet- 186/uL, urea-26 mg/dL, creatinine-0.6 mg/dL, serum Na-131 mmol/L, serum K-4.5 mmol/L, AST-37 U/L, ALT 19-U/L, ALP-52 U/L, total bilirubin-1.2 mg/dL.
In order to further clarify the cause of obstruction a CECT abdomen was done in emergency which revealed grossly dilated large bowel loop with thickened edematous and hypo-enhancing walls with twisting of its mesentery and mesenteric vessels in left lumbar region and associated increase in mesenteric fat stranding and haziness suggestive of distal transverse colon volvulus with early signs of strangulation. (Figure 2).
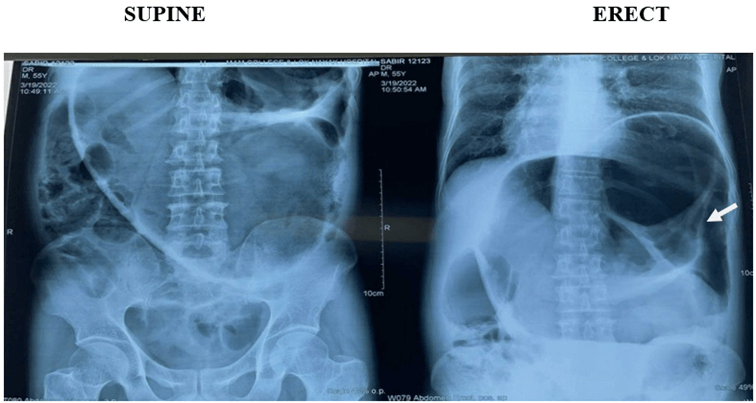
Figure 1: Abdomen x ray: Extremely dilated large bowel loop.
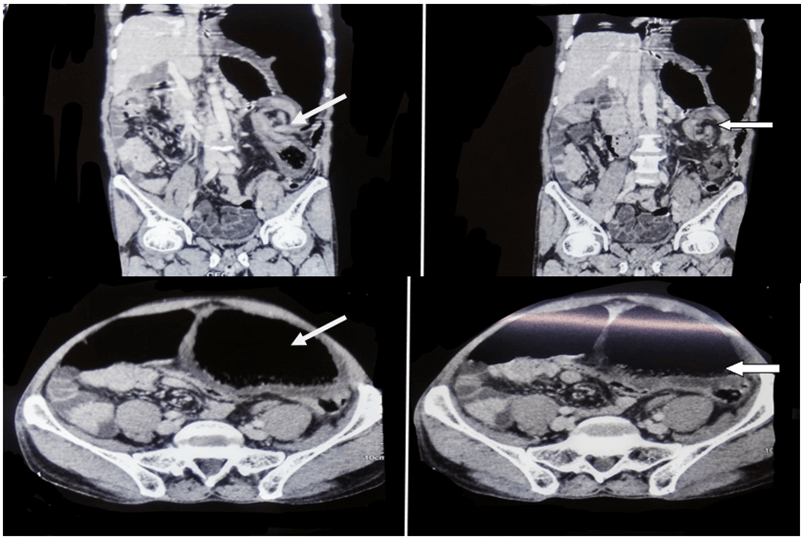
Figure 2: CECT abdomen showing dilated distal transverse colon with twisting of mesentery.
Patient was immediately taken for an emergency laparotomy. Intraoperatively anticlockwise rotation of transverse colon was seen with extremely distended and gangrenous proximal segment of transverse colon with fecal and gaseous content. The volvulus was detorsed in clockwise direction. A resection of the devitalized colonic segment was done with a Colo-colic anastomosis and a diversion loop ileostomy. (Figures 3 & 4).
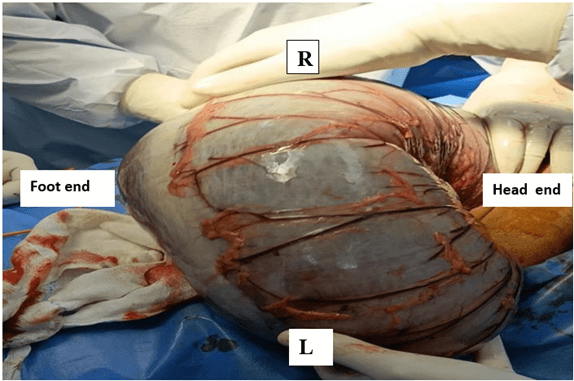
Figure 3: Detorsion of loop.
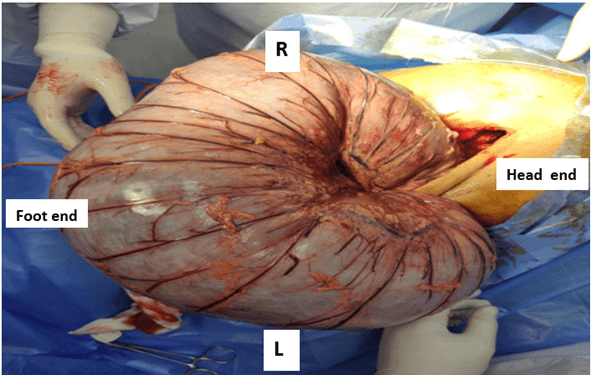
Figure 4: Final untwisted loop.
Biopsy of the resected segment showed large bowel of 60 cm with short-resected end measuring 2 cm and long resected end measuring 6 cm in diameter on gross examination and areas of acute ischaemia with extensive mucosal hemorrhage with viable ends on microscopic examination. Post operatively patient was allowed orally on POD 2, and gradually built up. The drains and foley's were removed on POD4. Patient was discharged on POD 8 in stable condition. Patient is currently on follow up and planned for stoma closure.
Discussion
Colonic volvulus constitutes only 3 to 5% of all cases of acute intestinal obstruction [2]. Any segment of the colon with a long loose mesentery, and a narrow base may get rotated [3]. Among them, transverse colon is involved only in 2 to 4% when compared to sigmoid colon (43 to 80%) and caecum (15 to 43%) [4, 5]. A male predominance is noticed [5]. An isolated volvulus of the transverse colon occurs extremely rarely.
Protective factors for transverse colon volvulus are short and broad mesentery and fixed hepatic and splenic flexure. Predisposing factors constitute congenital, physiological, and mechanical like earlier surgical procedures or bowel translocation, cancer, pregnancies, and congenital defects such as intestinal malrotation with an imperfect fixation of the posterior abdominal wall, megacolon, chronic constipation [6-8]. Clostridium difficile infection induced mucositis has been postulated to be associated with volvulus [9].
The twisting of the intestine around the mesenteric axis leads to blockade of the venous outflow because of the compression of the vessel in the early stage, and if left untreated then possibly, impaired arterial flow in later stage.
Transverse colon volvulus can present as sub acute onset or acute fulminant inflammation. In case of sub-acute onset there is massive abdominal distension with minimal pain abdomen no nausea, or vomiting, without any signs of peritonitis [2]. The leukocyte count is normal secondary to a lack of ischaemia at early stages. Patients having acute fulminating type of presentation have a sudden onset of severe abdominal pain, vomiting, little distension, signs of peritonitis and rapid clinical deterioration. Bowel sounds are initially hyperactive becoming absent later on due to peritonitis [2, 10]. Transverse colon volvulus is difficult to diagnose radiologically as there are no characteristic radiographic features, as in the case of volvulus of the sigmoid colon and caecum. The diagnosis is usually made intra-operatively. An early diagnosis can be achieved through computed tomography according to some studies [10].
It is worth mentioning that the co-occurrence of this disease with chilaiditi syndrome has been reported in the literature several times. This syndrome is characterized as a displacement of the hepatic flexure of the colon between the liver and the diaphragm. It is detected on x-ray and often confused with free air in the abdomen [11]. In contrast to sigmoid colon volvulus, an attempt at endoscopic decompression and drainage of the transverse colon volvulus is not recommended due to the high chances of necrosis and perforation [12]. Resection of the segment is the treatment of choice to prevent recurrence [2, 6]. In fact, detorsion alone or associated with colopexy has a higher rate of recurrence than resection [2, 6]. As the incidence of recurrence of volvulus after previous resection anastomosis varies between 22 and 36% some authors recommend performing a subtotal colectomy specifically in the presence of a megacolon, instead of partial resection of only the involved bowel segment [5]. This resection is carried out with or without primary anastomosis dependent on the viability of the remaining colon, the presence or absence of peritonitis, and general condition of the patient. In contrast to mortality rate in volvulus of sigmoid colon or caecum the mortality in volvulus of the transverse colon, is much higher 20% usually because of delayed diagnosis and treatment [13].
Conclusion
In conclusion, transverse colon volvulus is a rare but potentially life-threatening condition that requires prompt diagnosis and management. It is important for clinicians to consider this diagnosis in patients presenting with acute intestinal obstruction and abdominal distension. Abdominal computed tomography (CT) plays a crucial role in early detection and assists in determining the appropriate therapeutic approach. Surgical intervention remains the treatment of choice, with segmental resection and anastomosis being the preferred method to prevent recurrence. Although rare, transverse colon volvulus carries a higher mortality rate compared to other forms of colonic volvulus, emphasizing the importance of timely diagnosis and intervention. Continued vigilance and awareness of this condition are necessary for successful outcomes in managing this twist of a lifetime.
Article Info
Article Type
Case ReportPublication history
Received: Sat 21, Oct 2023Accepted: Mon 20, Nov 2023
Published: Wed 29, Nov 2023
Copyright
© 2023 Anubhav Vindal. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2023.04.01
Figures & Tables
References
1.
Hasnaoui H, Laytimi
F, Elfellah Y, Mouaqit O, Benjelloun EB, et al. (2019) Transverse colon
volvulus presenting as bowel obstruction: a case report. J Med Case Rep
13: 156. [Crossref]
2.
Sparks DA, Dawood
MY, Chase DM, Thomas DJ (2008) Ischemic volvulus of the transverse colon: A
case report and review of literature. Cases J 1: 174. [Crossref]
3.
Schwartz SI,
Brunicardi FC, Andersen DK, Billiar TR, Dunn DL et al. (2015) Schwartz’s
principles of surgery. McGraw-Hill Education.
4.
Valsdottir E, Marks
JH (2008) Volvulus: small bowel and colon. Clin Colon Rectal Surg 21: 91-93.
[Crossref]
5.
Booij KA, Tanis PJ,
Van Gulik TM, Gouma DJ (2009) Recurrent volvulus of the transverse colon after
sigmoid resection. Int J Colorectal Dis 24: 471-472. [Crossref]
6.
Ciraldo A, Thomas
D, Schmidt S (2000) A case report: transverse colon volvulus associated with
chilaiditis syndrome. Internet J Radiol 1.
7.
Tobinaga S, Morinaga
A, Sajima S, Kanazawa N, Yoshida T (2004) Transverse to descending colon
volvulus and megacolon with mesenterium commune: report of a case. Surg
Today 34: 875-877. [Crossref]
8.
Deshmukh SN, Maske
AN, Deshpande AP, Shende SP (2010) Transverse colon volvulus with chilaiditis
syndrome. Indian J Surg 72: 347-349. [Crossref]
9.
Yaseen ZH, Watson
RE, Dean HA, Wilson ME (1994) Case report: transverse colon volvulus in a
patient with Clostridium difficile pseudomembranous colitis. Am J Med Sci
308: 247-250. [Crossref]
10.
Liolios N, Mouravas
V, Kepertis C, Patoulias J (2003) Volvulus of the transverse colon in a child:
A case report. Eur J Pediatr Surg 13: 140-142. [Crossref]
11.
Matsushima K,
Suzuki Y (2006) Transverse colon volvulus and associated Chilaiditi’s syndrome.
Am J Surg 192: 203-204. [Crossref]
12. Elizondo ME, Arratíbel JA (2002) Colonic volvulus. Rev Esp Enferm Dig 94: 201-210. [Crossref]
13. Huerta S, Pickett ML, Mottershaw AM, Gupta P, Pham T (2023) Volvulus of the Transverse Colon. Am Surg 89: 1930-1943. [Crossref]