The Novel Use of the Amplatzer Occlusion Device to Aid in the Treatment of Massive Hemoptysis
A B S T R A C T
Massive hemoptysis is generally used to describe the expectoration of a large amount of blood and/or a rapid rate of bleeding, although the precise thresholds that constitute massive hemoptysis are controversial. Unfortunately, few options exist for the treatment of active bleeding from benign airway lesions. This case report highlights a challenging clinical situation where placement of an Amplatzer occlusion device over a proximal bleeding vessel resulted in cessation of hemorrhage until vascular embolization could be performed. The use of the Amplatzer occlusion device within the airways can be an effective intervention to aid in the treatment of massive hemoptysis.
Keywords
Bronchoscopy, Hemoptysis, Amplatzer
Introduction
Hemoptysis is characterized as coughing of blood from the airways or lungs. Massive hemoptysis is generally used to describe the expectoration of a large amount of blood and/or a rapid rate of bleeding, although the precise thresholds that constitute massive hemoptysis are controversial [1]. Hemoptysis can be life-threatening and may result from various etiologies, the most common causes being inflammatory airway diseases and lung cancer. Other common causes of hemoptysis include tracheobronchitis, pneumonia, foreign body ingestion, congestive heart failure, tuberculosis, severe trauma, and autoimmune conditions. Despite the gravity of the condition, no underlying etiology is identified in approximately half of the cases of hemoptysis [2]. If left untreated or undiagnosed, hemoptysis can result in death.
In the presented case, a 17-year-old male with a history of congenital pulmonary atresia and hypoplastic right heart syndrome corrected in the past via Fontan procedure was admitted to the hospital for massive hemoptysis. The etiology of the hemoptysis was determined to result from a bleeding superficial collateral bronchial artery vessel located in the proximal segment of the left lower lobe bronchus. Traditional attempts to control the bleeding were attempted, including vascular embolization and balloon occlusion, but were unsuccessful in controlling the ongoing hemorrhage. In order to stop the active bleeding from the proximal collateral vessel, an Amplatzer vascular occlusion device was successfully deployed into the segmental airway to cover the bleeding vessel and control active bleeding. Definitive treatment was performed using bronchial artery embolization.
Case Presentation
A 17-year-old male with congenital pulmonary atresia and hypoplastic right heart syndrome status post Blalock-Taussing (BT) shunt, Glenn, and Fenestrated Fontan procedure was admitted for respiratory distress secondary to repeated episodes of hemoptysis. His only home medication was daily low dose aspirin. Chest computer tomography scan on admission revealed a dense consolidation within the left lower lobe consistent with pulmonary hemorrhage. Massive hemoptysis developed shortly after admission resulting in intubation and assessment by interventional radiology for potential vascular embolization. When the bleeding vessel was not able to be identified through vascular angiography, rigid bronchoscopy was performed in the interventional radiology suite to assess endobronchial treatments for the active bleeding.
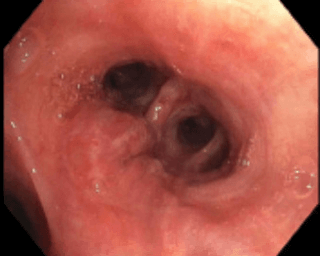
Figure 1: Hypertrophied collateral blood vessel in the left lower lobe bronchus.
Following clot aspiration, the source of bleeding was identified as a hypertrophied superficial vessel in the proximal aspect of the anteromedial segment of the left lower lobe. Figure 1 This vessel was likely due to collateralization resulting from his underlying cardiac condition and cardiac surgery. While balloon occlusion of the anteromedial segment of the left lower lobe resulted in hemostasis, bleeding recurred when the balloon was deflated. In an effort to compress the bleeding vessel and isolate the airway segment responsible for the bleeding, a 6mm Amplatzer vascular occlusion device was inserted into the bleeding sub-segment under direct bronchoscopic visualization. Figure 2 Placement of the Amplatzar device resulted in complete occlusion of the segmental airway and cessation of bleeding. The patient was extubated without difficulty and was observed in the hospital for 48 hours prior to discharge.
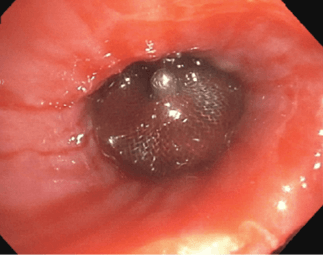
Figure 2: Successful endobronchial placement of Amplatzer device over bleeding vessel.
The patient returned to the interventional radiology suite two weeks later and was found to have multiple systemic collaterals identified including hypertrophied collaterals to the left lower lobe bronchus. These collaterals were embolized with 300-500 um embosphere particles. Embolization was then directed into the inferior branch arising from the lower left bronchial arterial trunk. Angiography confirmed a large arterial branch with significant blood flow to the area of the Amplatzer plug. This branch was super selectively embolized using a combination of 303/100-500 um embosphere particles. One week later, under rigid bronchoscopy, the Amplatzer device was removed without complication or further bleeding.
Discussion
This case report highlights a challenging clinical situation where placement of an Amplatzer occlusion device over a proximal bleeding vessel resulted in cessation of hemorrhage until vascular embolization could be performed. Use of bronchial blockers are notorious for migration and dislodgement following insertion and would necessitate intubation. The Amplatzer occlusion device is a specific form of transcatheter instrument used for providing minimally invasive treatment of cardiac related complications or defects. The Amplatzer occlusion device has been exclusively associated with providing closure to malformations of atrial septal defects and patent foramen ovale [2]. These specific instruments consist of a prefitted, double-disked frame, covered commonly with metal mesh that is inserted via catheter into the target site. Once inserted, the disks proceed to self-expand to pack the defect, while also stimulating routine cell growth around the affected area. In this case of massive hemoptysis, the Amplatzer occlusion device was successfully deployed under direct vision over the bleeding proximal vessel. Expansion of the mesh Amplatzer occlusion device created a selective airway plug resulting in persistent pressure on the vessel with a tamponade effect. Additionally, the Amplatzer occlusion device was used as a reference point during bronchial artery embolization to identify the bleeding vessel. Finally, following definitive therapy, the Amplatzer occlusion device was easily removed via rigid bronchoscopy.
Control of active bleeding during hemoptysis should be done promptly to assure appropriate management prior to severe, and possibly fatal, complications. Once a stable airway is achieved, the site and cause of the bleed must be explored bronchoscopically. Unfortunately, few options exist for the treatment of active benign bleeding from airway lesion. Use of bronchial blockers and selective mainstem intubation may temporize bleeding but are not long-term solutions. Hemoptysis resulting from malignant airway lesions can often be controlled with the use of thermal therapies such as electrocautery, argon plasma coagulation (APC), and radiofrequency ablation (RFA). When endobronchial therapy is not possible, use of angiography with subsequent bronchial artery embolization should be considered [3]. In life threatening situations when all minimally, invasive options have been exhausted, surgical intervention may be necessary [4].
The use of the Amplatzer occlusion device within the airways can be an effective intervention to aid in the treatment of massive hemoptysis. Few bronchoscopic devices are available for selective, segmental occlusion of airways in the setting of massive hemoptysis. The ease of placement and removal make the use of the Amplatzer occlusion device convenient to stabilize bleeding prior to definitive therapy such as bronchial artery embolization or surgery.
Article Info
Article Type
Case ReportPublication history
Received: Sat 28, Dec 2019Accepted: Fri 17, Jan 2020
Published: Thu 30, Jan 2020
Copyright
© 2023 Amit K. Mahajan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.JSCR.2020.01.01
Figures & Tables
References
- Ibrahim WH (2008) Massive haemoptysis: the definition should be revised. Eur Respir J 32: 1131-1132. [Crossref]
- Ittrich H, Bockhorn M, Klose H, Simon M (2017) The Diagnosis and Treatment of Hemoptysis. Deutsches Arzteblatt Int 114: 371-381. [Crossref]
- Rémy J, Voisin C, Dupuis C, et al. (1974) Traitement des hémoptysies par embolisation de la circulation systémique. Ann Radiol (Paris) 17: 5-16.
- Jean-Baptiste E (2000) Clinical assessment and management of massive hemoptysis. Crit Care Med 28: 1642-1647. [Crossref]