Testicular Torsion with a Twist
A B S T R A C T
Polyorchidism is a rare testicular malformation in children but has high propensity for torsion. We present a child with polyorchidism who presented with torsion testis and discuss the types and management of the polyorchidism.
Keywords
Polyorchidism, supernumerary testis, torsion
Introduction
Polyorchidism is a rare anomaly. Its presentation can be due to the associated maldescent, hernia or torsion. It must be considered in the differential diagnosis of a paratesticular mass.
Case Report
A 2-year-old boy was brought to the emergency room with three hours history of severe scrotal and lower abdominal pain which prevented him from walking. There was no history of trauma, insect bite or any urinary complaint. On examination he was afebrile. There was obvious swelling of his left hemiscrotum. The left testis was tender, enlarged, transversely lying and placed higher than the right. The left testis and epididymis were not separately palpable. The right scrotum, testis and epididymis were normal. The pain could not be relieved on elevation of the testis.
On palpating the left testis under general anaesthesia, a swelling was noted just above the testis. Exploration revealed the testis to be enlarged and congested after having undergone a 180-degree torsion (Figure 1).
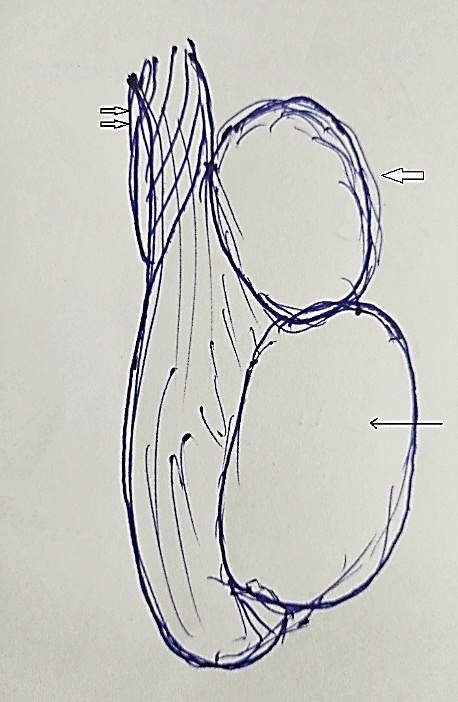
Figure 1: Drawing of operative finding showing supernumerary testis (thick arrow) above normal right testis (thin arrow) adherent to cord and 180-degree torsion (double arrows).
The testis recovered following derotation, warm compresses and 100% oxygen. A paratesticular mass measuring 5 x 5 x 7 mm was seen closely adherent to the vas. The mass was excised in toto preserving the vas deferens and left 3-point testicular fixation was done. In view of a possible neoplastic nature of the mass, the opposite testis was not explored. Right testicular fixation was planned later following the availability of histology findings. The boy made a smooth post-operative recovery and was discharged on the next day.
The histopathology report revealed the mass to be testicular tissue with absence of dysplastic or malignant cells. He underwent a planned right testicular fixation and remains well since.
Discussion
Polyorchidism is a rare anomaly, defined as the presence of more than two testicles. Around 150 cases with histological confirmation have been reported in the literature [1]. The majority of cases were triorchidism with occasional bilateral duplication [2]. Most of them were discovered in young adults [1, 3]. The supernumerary testis is most often located in the left side of the scrotum, as in this patient. It has been hypothesized that the left testis may be more prone to subdivision because of its greater size and different vascular topographic anatomy compared to the right testis [4].
Polyorchidism has been classified in different ways. Leung classified polyorchidism on the basis of embryologic development [5]. Singer et al. classified them based upon anatomical and functional potential [6]. Bergholz et al. proposed a more inclusive classification for standardisation of diagnosis and management depending on reproductive potential [7].
A supernumerary testis being drained by a vas deferens is Type A and which is not is Type B
A1- supernumerary testis has its own epididymis and vas (17%)
A2 - supernumerary testis has its own epididymis but shares a common vas (14%)
A3- supernumerary testis has a shared epididymis and a common vas (27%)
B1 - supernumerary testis has its own epididymis (10%)
B2 - supernumerary testis does not have its own epididymis (8%)
Our patient falls in B2.
The majority of supernumerary testes were found in the scrotal region (66%), followed by inguinal (23%) and abdominal (9%) positions [1]. The testicular anatomy in polyorchidism highly predisposes to testicular torsion. Because abnormal fixation of the testes by the tunica vaginalis tends to be bilateral, it is advocated that testicular fixation of the contra lateral testis is mandatory to avoid possible torsion. Common anomalies associated with polyorchidism are maldescent of the supernumerary testes (15%–50%) and inguinal hernia (30%). Others include testicular torsion (13%), hydrocele (9%), varicocele (< 1%), hypospadias (< 1%), anomalous urogenital union (< 1%), and malignancy (< 1%) [8]. Although it has been reported that incidence of cancer is less than 1% with polyorchidism, according to Giyanani et al. the actual collective incidence among the reported series is 6.25% [9].
Conclusion
Increased association of testicular torsion in polyorchidism makes greater understanding of this rare congenital anomaly important in surgical practice.
Disclaimers
None.
Competing Interests
None.
Article Info
Article Type
Case ReportPublication history
Received: Wed 01, Jul 2020Accepted: Fri 07, Aug 2020
Published: Wed 12, Aug 2020
Copyright
© 2023 Lakshmi Sundararajan. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.AJSCR.2020.03.08
Figures & Tables
References
- Robert Bergholz, Katharina Wenke (2009) Polyorchidism: A meta-analyses. J Urol 182: 2422-2427. [Crossref]
- A Hassan, S El Mogy, T Mostafa (2008) Triorchidism: a case report and review of similar conditions. Andrologia 40: 265-269. [Crossref]
- Robert Spranger, Marcel Gunst, Michael Kühn (2002) Polyorchidism: A strange anomaly with unsuspected properties. J Urol 168: 198. [Crossref]
- W A Wilson, J Littler (1953) Polyorchidism; a report of two cases with torsion. Br J Surg 41: 302-307. [Crossref]
- A K Leung (1988) Polyorchidism. Am Fam Physician 38: 153-156. [Crossref]
- B R Singer, J G Donaldson, D S Jackson (1992) Polyorchidism: functional classification and management strategy. Urology 39: 384-388. [Crossref]
- Robert Bergholz, Bernward Koch, Tilmann Spieker, Kerstin Lohse (2007) Polyorchidism: a case report and classification. J Pediatr Surg 42: 1933-1935. [Crossref]
- Alexander K C Leung, Andrew L Wong, C Pion Kao (2003) Duplication of the testis with contralateral anorchism. South Med J 96: 809-810. [Crossref]
- V L Giyanani, J McCarthy, D D Venable, J Terkeurst, M Fowler (1987) Ultrasound of polyorchidism: case report and literature review. J Urol 138: 863-864. [Crossref]