Sublingual Swelling Masquerades a Ranula: A Case Report and Review of the Literature
A B S T R A C T
Epidermoid cyst in the floor of mouth is a very rare non-neoplastic cyst lined by squamous epithelium. Here is a case report of a 17-year-old female who presented with a slow growing swelling in the floor of mouth with difficulty in breathing and swallowing from past 4 months. A clinical diagnosis of ranula was made. Biopsy and subsequent histopathological evaluation revealed it as epidermoid cyst. Thus, epidermoid cyst of the floor of mouth can mimic ranula in its clinical presentation. Therefore, histopathologic evaluation is critical in making definitive diagnosis in such scenarios. A detailed account of clinical, radiological and histopathological evaluation has been presented.
Keywords
Cysts, floor of mouth, epidermoid cyst, oral cavity, ranula
Introduction
Epidermoid cyst is a rare, developmental cystic malformation, benign in nature encountered throughout the body where embryonic elements amalgamate together. The majority of cases are reported in testes and ovaries (80%) [1]. However, only 7% cases have been reported in head and neck with about 1.6% in oral cavity, which accounts for 0.01% of all oral cysts [2]. Till date only 29 case reports of epidermoid cyst in the floor of mouth have been cited in the literature. Here we report a case which clinically as well as radiographically mimicked sublingual ranula but histopathologically turned to be epidermoid cyst. It was thus an eye opener for the oral surgeon as well as oral pathologist alike.
Case Report
A 17-year-old female reported to the outpatient department seeking consultation for a swelling in the floor of her mouth present since past 4 years with no relevant personal or family history. She was asymptomatic till past 4 months when the swelling gradually increased in size that led to difficulty in swallowing and breathing. On extraoral examination, no gross facial asymmetry was noted. There was no palpable cervical lymphadenopathy or fever. Intraorally, a solitary well defined dome shaped swelling approximately 5 cm in diameter, involving the entire floor of the mouth was noted. The swelling had displaced the tongue upwards such that the soft palate was not visible (Figure 1A). On palpation the swelling was non tender, afebrile, non-reducible, fluctuant and smooth in texture. The mucosa overlying the swelling was apparently normal with no signs of inflammation. MRI revealed a well-defined lobulated lesion in the floor of the mouth on right side which bulged anteriorly towards left side, and displaced the tongue to left side (Figure 1B). Initial diagnosis was of a ranula, due to its higher prevalence, clinical appearance and its location in the midline. The lesion was surgically excised in toto and the specimen was sent for histopathological interpretation.
Macroscopically, the specimen appeared to be spherical, 3 × 3 cm, yellowish pink in colour, encapsulated, soft in consistency and cystic in nature (Figure 1C). On sectioning, the cavity was filled with yellowish cheese like material (Figure 1D). The tissue sections revealed 2-3 cell thin cystic lining of stratified squamous epithelium. Cystic content showed abundant lamellar keratin. Intervening stroma was scanty and fibrous with no evidence of hair follicles or sebaceous gland (Figures 2A & 2B). The final diagnosis of epidermoid cyst in the floor of mouth was made which masqueraded clinically as sublingual ranula.

Figure 1: A) Photograph showing swelling on the floor of mouth, with tongue displaced upwards. B) Revealed well defined swelling involving the floor of the mouth. C) Macroscopic view of the excised specimen. D) Cystic cavity filled with yellowish cheese like material.
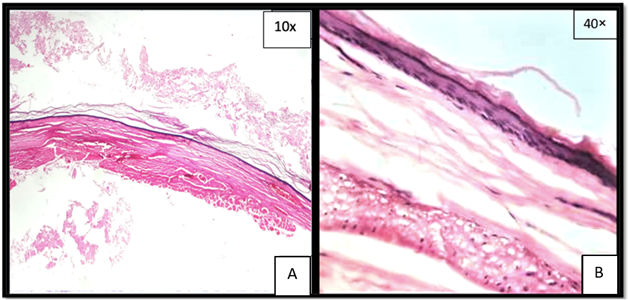
Figure 2: A & B) Photomicrograph revealing cystic lining composed of stratified squamous epithelium with lumen showing lamellar keratin.
Discussion
Epidermoid cysts are developmental pathologies derived from aberrant ectodermal tissue [1]. A number of theories have been put forward to explain its etiopathogenesis which includes: dysontogenic, traumatic, and thyroglossal anomaly [3]. The most frequently involved site of head and neck region is the orbit followed by calvarial diploic and intracranial spaces. Rarely, tongue, buccal mucosa, parotid gland, lower lip, tonsils and intraosseous involvement has been documented [4, 5].
The epidermoid cysts of the floor of the mouth are considered as scarce. Shore reported only four cases of sublingual epidermoid cyst in a review of 54,000 cases [6]. These cysts can occur in any age group, right from birth (congenital) to 72 years, with male preponderance. Anatomically cysts in the floor of mouth have been categorized according to their relation to the muscles: a) Sublingual cyst (medial genioglossus): these are above mylohyoid and genioglossus muscles, clinically presenting as swelling in the floor of the mouth. b) Sub mental cyst (medial geniohyoid): between mylohyoid and geniohyoid, presenting as swelling below the chin giving classical “double chin” or “hourglass” appearance and c) lateral cysts: these are present in sublingual space, may penetrate mylohyoid muscle and occupy both the spaces [4]. Clinically, epidermoid cysts are painless, slow growing lesion with doughy consistency, often soft and well encapsulated without any associated lymphadenopathy [7]. When they expand in size superiorly into oral cavity, they push the tongue upwards and backwards resulting in dysphagia, dysphonia and dysnoea [8]. These cysts can be associated with certain hereditary syndromes like Gardner syndrome or Lowe syndrome (Oculo Cerebro Renal Lowe syndrome) [3].
However, in the present case no symptom associated with syndrome was seen. Histologically, mayer defined three variants: epidermoid (simple), dermoid (compound) and teratoid (complex). Epidermoid cyst is always lined by stratified squamous epithelium without dermal appendages within the underlying connective tissues. A dermoid cyst in addition contains dermal appendages like hair follicles, hairs, sebaceous and sweet glands. The teratoid cyst exhibit lining and wall with tissue structures derived from all three germ layers; ectoderm, mesoderm and endoderm. The lumen of all three types of cysts is filled with cheesy yellowish content formed by shed keratin and sebaceous material. Epidermoid cysts are composed only of connective tissue wall lined on the inner surface by a thin layer of stratified squamous epithelium, usually showing keratinization. Desquamated keratin may fill the cystic cavity giving it a semisolid consistency.
The differential diagnosis of cystic lesions in the floor of mouth are ranula, unilateral or bilateral blockage of wharton’s duct, thyroglossal cyst, cystic hygroma, branchial cleft cyst, infection of sublingual and submandibular gland, and tumors in this region etc. Radiographic diagnosis is mostly made by MRI (mostly), CT scan or USG (least) to delineate the extent of swelling [8]. In most of the cases, initial diagnosis was of ranula is given due to typical clinical and radiological presentation which is similar to the present case. However, histopathology is the mainstay for final diagnosis of epidermoid cyst.
Standard treatment is complete surgical enucleation. Prognosis is very good with low incidence of recurrence. Malignant transformation of dermoid/epidermoid cyst is exception [13]. Devine and Jones described first case of malignant transformation of a sublingual dermoid cyst to squamous cell carcinoma [8]. It is pertinent to be aware about them as the treatment plan varies accordingly.
Conclusion
The main aim to report this case was to highlight the rarity of epidermoid cyst in the floor of mouth. Ample understanding and vigilance about this slow growing painless mass is essential not only due to its symptoms but also due to its malignant potential.
Funding
None.
Conflicts of Interest
None.
Author Contributions
The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
Article Info
Article Type
Case Report and Review of the LiteraturePublication history
Received: Tue 15, Aug 2023Accepted: Mon 28, Aug 2023
Published: Fri 08, Sep 2023
Copyright
© 2023 Ridhi Bhola. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.DOBCR.2023.01.03
Figures & Tables
References
1.
Tandon PN, Gupta DS
(2014) Epidermoid cyst in the floor of mouth with sub mental component. J Maxillofac Oral Surg 13: 59-62. [Crossref]
2.
Kandogan T, Koç M,
Vardar E, Selek E, Sezgin O (2007)
Sublingual epidermoid cyst: a case report. J
Med Case Rep 1: 87. [Crossref]
3.
Dabán RP, Díez EG,
Navarro BG, López López J (2015) Epidermoid cyst in the floor of the mouth of a
3-year-old. Case Rep Dent 2015: 172457. [Crossref]
4.
Lyngdoh TS, Konsam
R, Venkatesh MA, Aggarwal S (2010) Giant sublingual epidermoid cyst - An
unusual case report. Indian J Surg 72: 318-320. [Crossref]
5.
Nee TS, Ramli R,
Athar PPSH (2015) Sublingual epidermoid cyst resembling sublingual ranula: a
case report. Archives of Orofacial
Sciences 10: 46-51.
6.
Jham BC, Duraes GV,
Jham AC, Santos CR (2007) Epidermoid cyst of the floor of the mouth: a case report.
J Can Dent Assoc 73: 525-528. [Crossref]
7.
Qamar Z, Ikram K,
Fatima T (2016) Sublingual epidermoid cyst mimicking as plunging ranula-A case
report. International Journal of Dental
Science and Research 3:
22-25.
8.
Baliga M, Shenoy N,
Poojary D, Mohan R, Naik R (2014) Epidermoid cyst of the floor of the mouth. Natl J Maxillofac Surg 5: 79-83. [Crossref]
9. Patil K, Mahima VG, Malleshi SN (2009) Sublingual epidermoid cyst: a case report. Cases J 2: 8848. [Crossref]
10. Sadigov E., Afendiyev Y, Rahimov C, Davudov M (2018) Sublingual Epidermoid Cyst Simulating a Plunging Ranula: 2 Rare Case Reports. POJ Dent Oral Care 2: 1-4.