Simultaneous Bilateral Rupture of the Quadriceps Tendon after Minor Trauma in a Patient Receiving Hemodialysis: A Rare Variant to an Uncommon Injury
A B S T R A C T
A spontaneous and simultaneous complete bilateral ruptures of the knee extensor system is a rare entity, and only few cases have been reported in literature. It is a rare occurrence After minor trauma. Therefore, an investigation should be focused on identifying certain medical predisposing conditions including chronic diseases and long-term use of certain drugs. Surgical repair is a treatment of choice. This article describes the case of a 36-year-old patient with renal failure requiring hemodialysis for the past 7 years, who sustained spontaneous bilateral rupture of quadricepital tendon diagnosed by bilateral ultrasound scan of the thighs and successfully managed by surgical repair using sutures passed through drilled holes in the patella. Post-operatively, the patient was immobilized with splints for 6 weeks before starting physiotherapy.
Keywords
Quadriceps tendon, bilateral rupture, chronic renal failure, surgical repair
Introduction
Bilateral forms of quadriceps tendon rupture are rare and predominantly occurs after major trauma in younger patients or as the result of tendon weakening due to obesity and arteriosclerosis-induced fibrotic changes or previous injury [1]. We report an unusual case of simultaneous bilateral quadriceps tendon rupture after simple fall at home in a patient with renal failure diagnosed by bilateral ultrasound scan of the thighs, and successfully managed by surgical repair using sutures passed through drilled holes in the patella.
Case Report
A 36-year-old male with a history of renal failure requiring hemodialysis for the past 7 years and controlled hypertension, was presented to emergency room complaining of bilateral pain and a defect in the continuity of both quadriceps tendons upon palpation above the patella (Figure 1) following the history of a simple fall at home with impact on both knees. Clinical examination revealed incomplete active knee extension that was very painful and a gap in both suprapatellar regions (Figure1). Plain radiographs of both knees revealed a low riding of both patellae, and signs of suprapatellar ossification of the left knee (Figure 2). Bilateral ultrasound scan of the thighs confirmed the diagnosis of bilateral quadriceps tendon rupture (Figure 3). The treatment consisted of Bilateral quadriceps surgical repairs using mid-line incisions over the knees. The peri-operative findings were complete rupture of the tendons, bilaterally from the superior pole of the patella (Figure 4). The ruptured ends were freshened and repaired using Vicryl 2-0 sutures through drill holes in the patella to the tendons, reinforced by a surgy using vicryl 2-0 (Figure 5). The operative follow-up was simple; the patient was immobilized with splints for 6 weeks before starting physiotherapy.
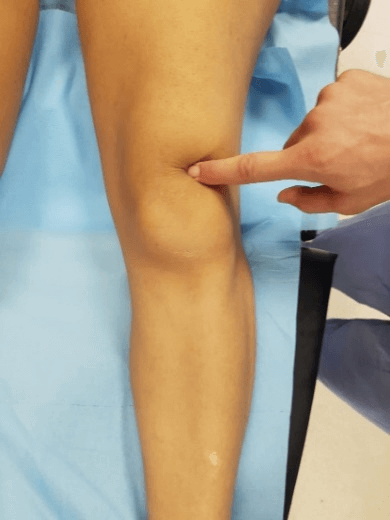
Figure 1: Palpation showing depression above the patella (gap test).
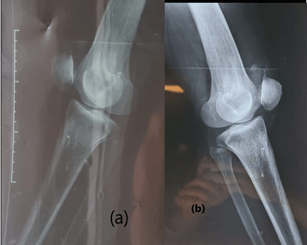
Figure 2: Plain radiographies show low riding of both patellae and signs of suprapatellar ossification of the left knee (b).
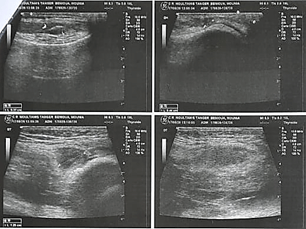
Figure 3: Ultrasound scans of the thighs showing a complete bilateral rupture of the tendon.

Figure 4: Intraoperative pictures of the ruptured quadriceps tendons.
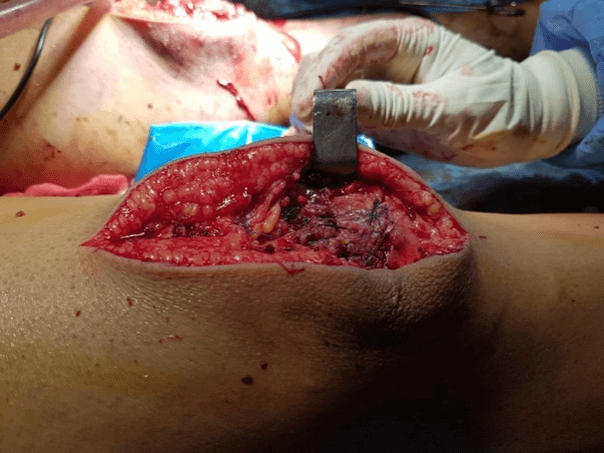
Figure 5: Quadriceps tendon reinserted through tendon-to-bone repair.
Discussion
Simultaneous bilateral rupture of the quadriceps tendon is considered very rare injury. Steiner and Palmer were the first to report a patient with simultaneous bilateral quadriceps tendon rupture in 1949 [2]. Some of the main causes are long term steroid usage, fluoroquinolone injections at local site or associated co-morbidities such as chronic renal failure, diabetes, obesity, hyperparathyroidism, endocrine disorders and gout, which via different mechanism lead to weakening of tendon, thereby predisposing it to rupture [3-5]. Quadriceps tendon rupture can occur by direct or indirect mechanisms after strong contraction of the quadriceps muscle while the knee is in semi flexion and the ankle is in plantar flexion [6].
Patients with quadriceps tendon rupture are typically unable to walk without assistance and tend to hold their knee in an extension position to relieve the pain [7, 6]. During examination, patients cannot actively extend their knees and often have a palpable gap above the patella, the so-called “sulcus sign” or “gap test” [8]. The triad of symptoms with painful swelling, palpable suprapatellar gap, and the inability to actively extend the knee is not obligatory and only found in about 60% of patients [9]. A differential diagnosis for patients unable to perform full active knee extension may include femoral nerve palsy, which might be traumatic or iatrogenic [10].
Radiographic views of the knee reveal only indirect signs of the lesion including soft tissue swelling above the kneecap, shadow in the tendon line, patellar spurs at the tendons insertion, and patella Baja. Calcification of the superior pole of the patella may indirectly indicate quadriceps tendinopathy, which is a predisposition to rupture [11]. Ultrasound confirms the quadriceps tendon rupture, but the interpretation of the results must be performed by a trained specialist. MRI is another sensitive diagnostic tool that can precisely locate the tear, determine which four layers of the quadriceps tendon are affected or whether the rupture is partial, and determine whether the retinaculum is torn [9].
Surgery based on reintegration has always been the standard treatment for fresh ruptures and therefore providing the best results [9]. Lighthart et al. studied quadriceps tendon strength after trans osseous suturing and tendon anchoring [12]. Accordingly, their results showed no difference between the two techniques. Delayed surgical repair has been associated with protracted physiotherapy, extension lag, inadequate flexion, and use of adaptive equipment, hence the value of early diagnosis and treatment [8].
After the operation, walking was permitted albeit with a splint keeping the knee extended for 4 to 6 weeks, which helps protect the reconstruction that has been described [13]. Most authors have reported good functional results, always with complete motion recovery and return to previous activities [12, 13]. a secondary rupture may occur but remains rarity [14].
Article Info
Article Type
Case ReportPublication history
Received: Mon 07, Dec 2020Accepted: Thu 17, Dec 2020
Published: Wed 30, Dec 2020
Copyright
© 2023 Asbai Mohamed. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Hosting by Science Repository.DOI: 10.31487/j.GSCR.2020.02.12
Figures & Tables
References
- Thaunat M, Gaudin P, Naret C, Beaufils P, Thaunat O (2006) Role of secondary hyperparathyroidism in spontaneous rupture of the quadriceps tendon complicating chronic renal failure. Rheumatology (Oxford) 45: 234-235. [Crossref]
- Steiner C, Palmer LH (1949) Simultaneous bilateral rupture of quadriceps tendon. Am J Surg 78: 752-755. [Crossref]
- Dhar S (1988) Bilateral, simultaneous, spontaneous rupture of the quadriceps tendon. A report of 3 cases and a review of the literature. Injury 19: 7-8. [Crossref]
- Mounasamy V, Chadderdon RC, McDaniel C, Willis MC Jr (2008) Bilateral synchronous quadriceps tendon rupture: a case report. Eur J Orthop Surg Traumatol 18: 63-67.
- Stephens BO, Anderson GV Jr (1987) Simultaneous bilateral quadriceps tendon rupture: a case report and subject review. J Emerg Med 5: 481-485. [Crossref]
- Hussain WM, Griesser MJ, McCoy BW, Parker RD (2015) Extensor mechanism injuries of the knee. DeLee & Drez’s Orthopaedic Sports Medicine. 4th. Philadelphia, PA, USA: Elsevier Saunders.
- Siwek CW, Rao JP (1981) Ruptures of the extensor mechanism of the knee joint. J Bone Joint Surg 63: 932-937. [Crossref]
- Walker L, Glick H (1989) Bilateral spontaneous quadriceps tendon ruptures: a case report and review of the literature. Orthop Rev 18: 867-871. [Crossref]
- Ilan DI, Tejwani N, Keschner M, Leibman M (2003) Quadriceps tendon rupture. J Am Acad Orthop Surg 11: 192-200. [Crossref]
- Thoms RJ, Kondrashov D, Silber J (2009) Iatrogenic femoral nerve palsy masquerading as knee extensor mechanism rupture. Am J Orthop (Belle Mead NJ) 38: 142-144. [Crossref]
- Hardy JR, Chimutengwende Gordon M, Bakar I (2005) Rupture of the quadriceps tendon: an association with a patellar spur. J Bone Joint Surg Br 87: 1361-1363. [Crossref]
- Lighthart WA, Cohen DA, Levine RG, Parks BG, Boucher HR (2008) Suture anchor versus suture through tunnel fixation for quadriceps tendon rupture: a biomechanical study. Orthopedics 31: 441. [Crossref]
- Ennaciri B, Montbarbon E, Beaudouin E (2015) Surgical management of acute quadriceps tendon rupture (a case report with literature review). Pan Afr Med J 22: 243. [Crossref]
- Stinner DJ, Orr JD, Hsu JR (2010) Fluoroquinolone-associated bilateral patellar tendon rupture: a case report and review of the literature. Mil Med 175: 457-459. [Crossref]